Anatomy
The inner thigh muscles (M adductor longus, M adductor brevis and M adductor magnus, M gracilis and M pectineus) all attach in the groin to the pubic bone.
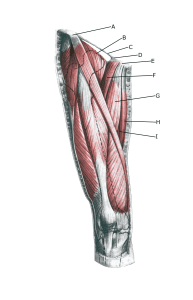 Thighs from the front:
Thighs from the front:
A. Spina iliaca anterior superior
B. M. iliopsoas
C. Lig. inguinal
D. Lig. gaps
E. Tuberculum pubicum
F. M. pectineus
G. M. adductor longus
H. M. gracilis
I. M. adductor magnus
Cause
Strain-related symptoms from the attachments of the inner thigh muscles in the groin (tendinopathy) occur with repeated repetitive repetitive stresses that exceed the strength of the tendon. This causes microscopic tears in the tendon and especially at the tendon attachment, resulting in “inflammation“.
The tendonitis is a warning that the training is too strenuous for the current muscle tendon, and if the load is not reduced, a rupture (“fiber”) and long-term changes can occur with a rehabilitation period of more than ½ year.
The adductor longus muscle, which feels like a firm string in the groin, is the most commonly injured of the inward-facing muscles. The muscle is particularly Injured in sports characterized by fast running activity with sudden changes of direction, a lot of strength training and modest agility training (football, ice hockey), while it is very rarely seen in sports characterized by agility (gymnastics).
Approximately 1/4 of all muscle injuries in football are related to the adductor longus. In some cases, symptoms can also involve the abdominal muscle attachment to the pubic bone and the pubic symphysis. In rare cases, the symptoms originate from the adductor brevis and magnus muscles in the groin.
Symptoms
Pain on pressure along the tendon and especially at the attachment of the pubic bone with aggravation when stretching and activating the muscle tendon (squeezing of stretched legs against resistance, isometric contraction).
In mild cases, a localized soreness is felt at the start of exercise, but the symptoms can often fade after a thorough warm-up and return after the sporting activity has stopped (“muscle strain”, “threatening fiber”, “tendonitis”).
In more severe cases, a sudden shooting pain is felt in the muscle (‘partial muscle rupture’, ‘fibre rupture’) and in the worst case, a violent snap is felt, after which it is impossible to use the muscle (‘total muscle rupture’). The following three symptoms are characteristic of muscle and tendon injuries: pain on palpation, during stretching and when contracting against resistance.
Examination
In mild cases, the diagnosis is made based on the clinical examination alone. Severe cases or cases that do not improve on treatment or sudden pain with affected muscle function (suspected total rupture) should be assessed by a professional for correct diagnosis and treatment.
If the examination reveals pain when pressing on the muscle tendon attachment in the groin and aggravation in the same place when stretching and activating the inner guides, there is little doubt about the diagnosis. In other cases, the diagnosis of groin pain can be extremely difficult and requires specialist medical assessment and ultrasound scans and possibly X-rays and MRI scans.
Treatment
As tendonitis of the inner thigh (M adductor longus) is one of the sports injuries most likely to take a long time (over six months), it is crucial that treatment starts as soon as the first symptoms are felt (and not after several months of increasing discomfort).
Treatment includes relief from pain-inducing activity, stretching and slowly increasing load within the pain threshold. Special emphasis is placed on strength training by activating the tendon while stretching (eccentric training) or slow heavy strength training (Beyer R, et al. 2015).
The treatment is the same if Injury is localized to the other inward muscles (adductors) in the groin.
If off-loading and long-term rehabilitation is unsuccessful, medical treatment may be considered in the form of an injection of adrenal cortex hormone around the inflamed part of the tendon. As adrenal hormone injection is always part of a long-term rehabilitation of a chronic injury, it is crucial that the post-injection rehabilitation process lasts several months to reduce the risk of recurrence and rupture. In severe cases, rehabilitation lasts for six months before maximum load in the form of running with direction changes is allowed. See generally, chronic tendonitis.
If no progress is made with rehabilitation and injection therapy, surgery may be considered. The long-term results of surgery are often disappointing. Successful conservative treatments for total ruptures have been described, but if the distance from the tendon to the bone attachment is more than a few centimeters, surgery is often offered.
The documentation of the quality of the different treatments for groin injuries is generally poor(Serner A, et al. 2015).
Complications
If the progression is not smooth, you should consider whether the diagnosis is correct Det vil ofte være nødvendigt at henvise til billeddiagnostiske undersøgelser, primært ultralydskanning og røntgen (eller MR-skanning).
In particular, the following should be considered:
- Osteoarthritis of the hip joint
- Tendonitis of the superficial hip flexor attachment
- Tendonitis of the deep hip flexor
- Outer jump hip
- Inner jump hip
- Fluid accumulation in the joint
- Fatigue fracture of the femoral neck
- Inguinal hernia
- Inflammation of the abdominal muscle attachment on
- Pubic bone
- Inflammation of the temporomandibular joint
- Nerve entrapment
- Inflammation of the anterior cruciate ligament
- Hip joint