Anatomy
The elbow joint is formed by the humerus and ulna. The other forearm bone (radius) forms a joint with the ulna (species radioulnaris proximalis). Around the elbow joint is a joint capsule and several reinforcing ligaments.
 Two major muscle groups of the forearm attach to the elbow, one on the outside (lateral epicondyle) and one on the inside (medial epicondyle), where in adolescents there is a growth zone (apophysis) that increases the risk of overuse symptoms. The forearm muscles that attach to the inside of the elbow flex (flex) and rotate (pronate) the hand. A ligament that stabilises the elbow (ulnar collateral ligament) attaches in the same place.
Two major muscle groups of the forearm attach to the elbow, one on the outside (lateral epicondyle) and one on the inside (medial epicondyle), where in adolescents there is a growth zone (apophysis) that increases the risk of overuse symptoms. The forearm muscles that attach to the inside of the elbow flex (flex) and rotate (pronate) the hand. A ligament that stabilises the elbow (ulnar collateral ligament) attaches in the same place.
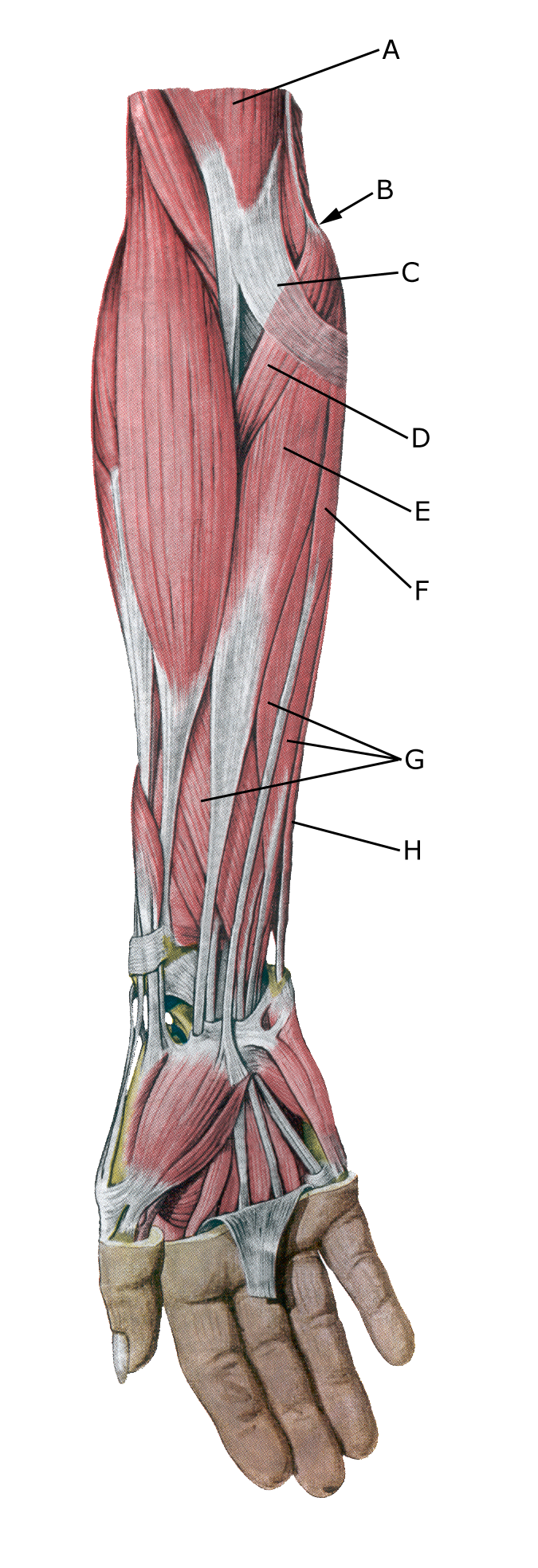
Forearm flexor muscles
A. M. biceps brachii
B. Epikondylus mediale
C. Aponeurosis m. bicipitis brachii
D. M. pronator teres
E. M. flexor carpi radialis
F. M. palmaris longus
G. M. flexor digitorum superficialis
M. flexor carpi ulnaris