Examination
Any athlete who suffers a blow to the head and subsequently complains of discomfort should immediately stop the sporting activity and be examined by a medical professional. In cases of loss of consciousness, unconsciousness or balance problems, the athlete should be removed from the field and assessed by a doctor or other authorised medical professional and should not return to sporting activity on the day of the injury.
If a sideline assessment does not indicate a concussion, a healthcare professional can assess whether the athlete can continue the sporting activity. If the athlete is allowed to continue, a follow-up assessment must be made to determine if there is a delay in the development of symptoms.
If there is no doctor or other medical professional present, the athlete should be assessed at the local hospital if concussion is still suspected.
All head injuries must be taken seriously, as in some cases, life-threatening bleeding or chronic damage can occur.

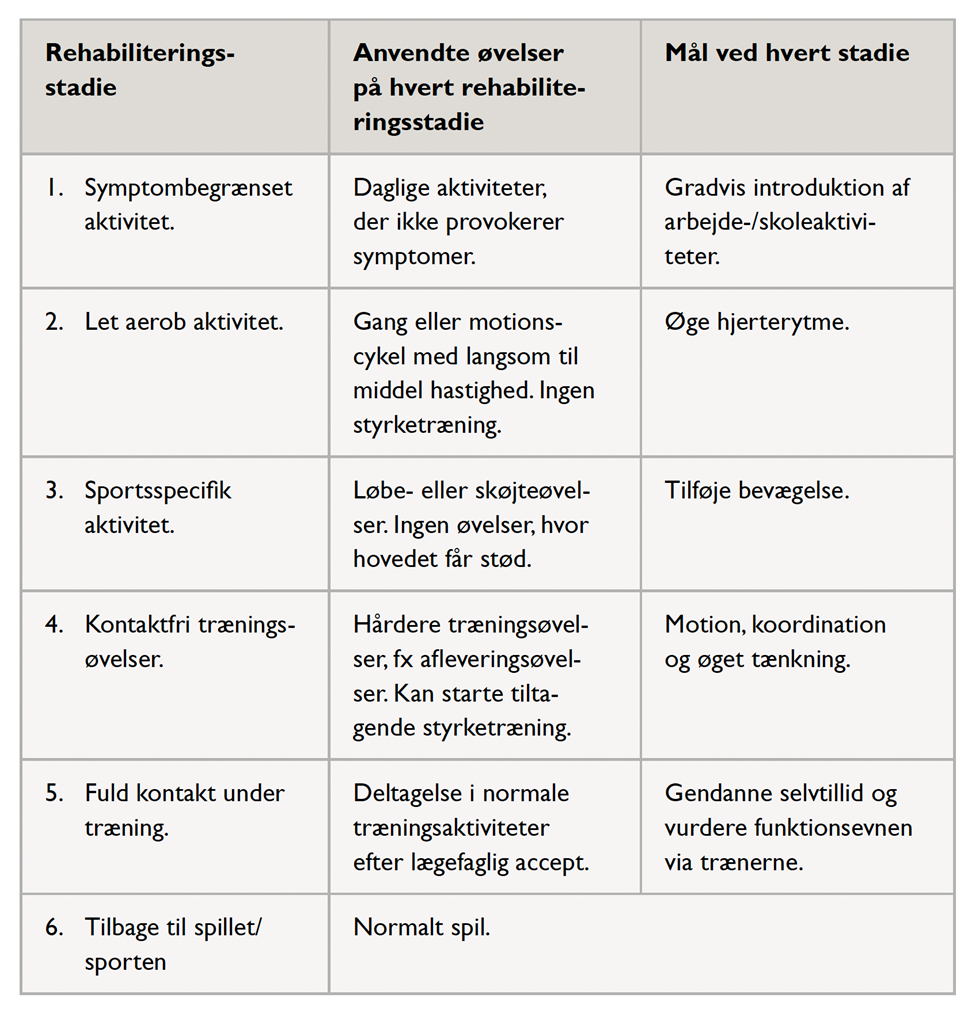
Rehabilitation, specific:
Rest and take it easy for 1–2 days. After that, training can be gradually resumed as shown in the diagram, provided the symptoms do not worsen. There should be at least 24 hours between each of the 6 steps.