Anatomy
The calf muscles are divided into three muscle groups (compartments) by strong muscle sheaths (fasciae). A anterior muscle compartment (containing the flexor muscles of the foot), a lateral muscle compartment (containing the peroneal muscles) and a posterior muscle compartment (containing the extensor muscles of the foot).
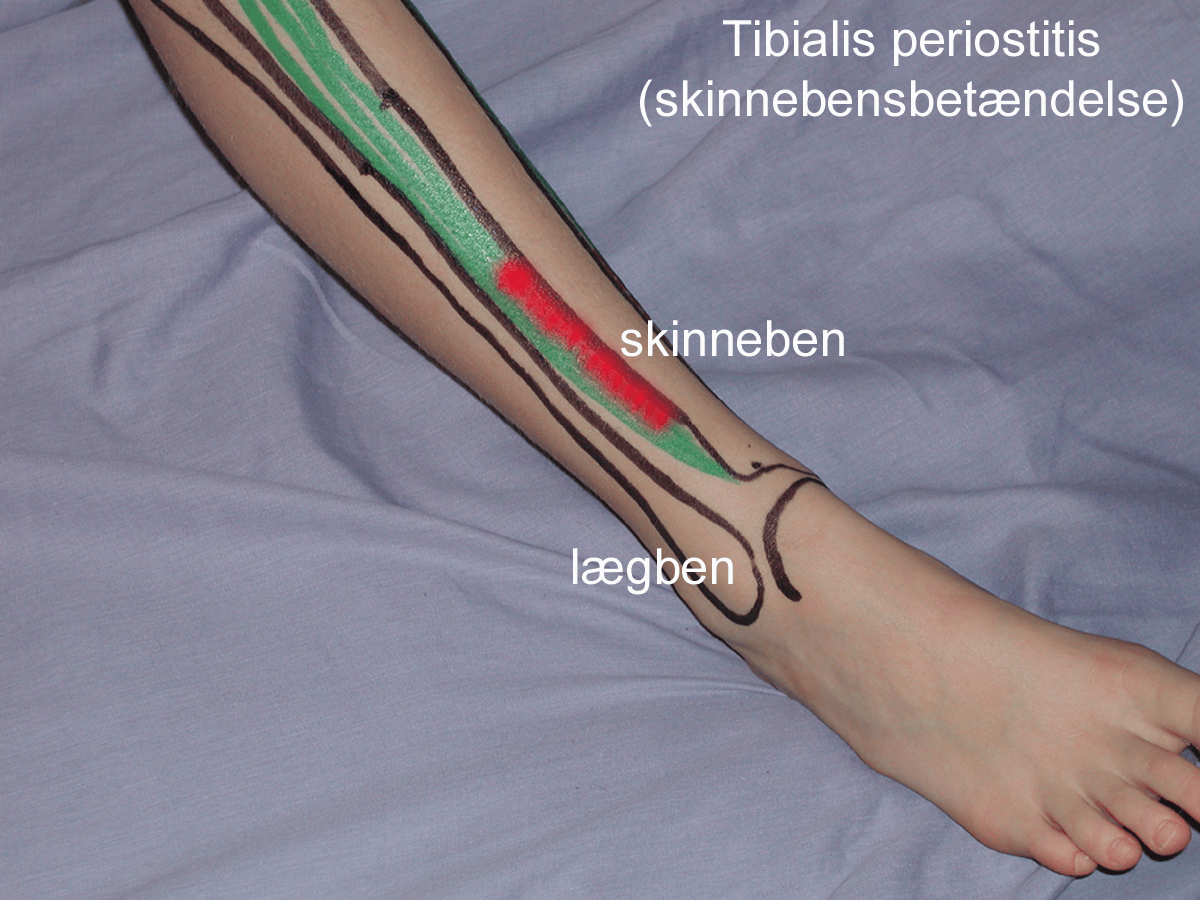
See image of Tibialis periostitis (shin splints – fibula)
{kind=link}
The large posterior muscle group’s muscle sheath attaches to the inner edge of the tibia, while the anterior muscle group’s muscle sheath attaches to the outer edge of the tibia.
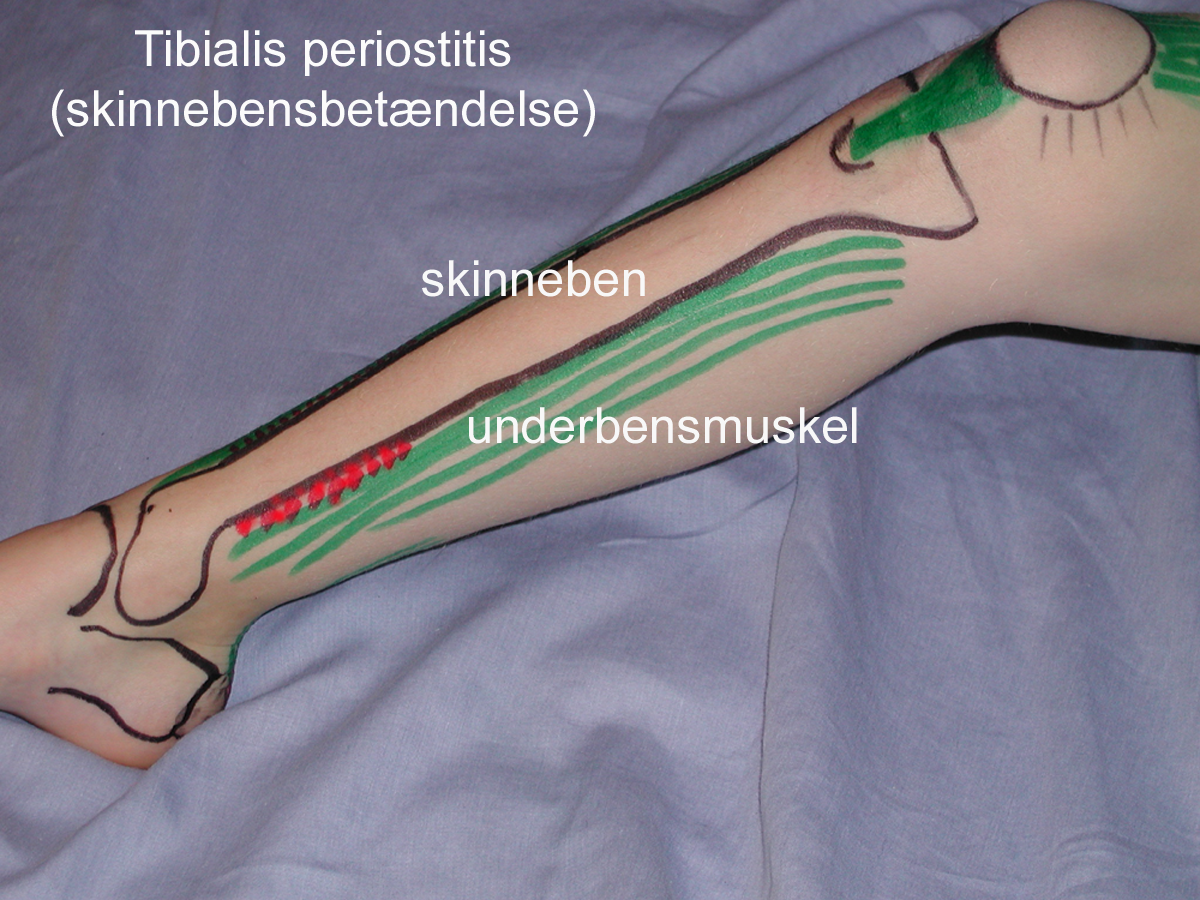
See image of Tibialis periostitis (shin splints – lower leg)
{kind=link}
Cause
If the training intensity increases too quickly with repetitive, repetitive loads (running, jumping, dancing) that exceed tissue strength, overload-related microscopic lesions and ‘inflammation’ can occur at the attachment of the muscle membrane on the tibial crest.
The condition is most common in runners with frequent changes of running surfaces. Pronounced pronation (where the foot ‘falls’ inwards when landing during running) is thought to increase the risk of internal (medial) shin splints.
Symptoms
Worsens with pressure and strain. Often improves temporarily after warming up. Pain on the inside edge of the tibia worsens when the ankle is stretched (flexion) against resistance and pain on the outside edge of the tibia worsens when the foot is bent up against resistance (extension).
The pain is usually localised to the lower 1/3 of the tibia and is often bilateral.
Examination
In mild cases, medical examination is not necessarily required and the diagnosis is usually made on clinical examination alone, where the pain is localised directly on the edge of the shin.
In cases of more pronounced pain or lack of progress despite relief, a medical examination is recommended to confirm the diagnosis and rule out fatigue fractures, among other things.
In some cases, it may be necessary to supplement with an X-ray, ultrasound scan or MRI scan.
Treatment
Treatment primarily includes relief from pain-inducing activity (running), stretching and slowly increasing rehabilitation within the pain threshold. It is crucial that good shock-absorbing shoes are used (Deshmukh NS, Phansopkar P. 2022).
Complications
If the progress is not smooth, a medical assessment should be carried out to ensure the diagnosis is correct and that there are no complications such as fatigue fractures.