Anatomy
The clavicle (clavicle) forms a joint with the sternum and the upper bony prominence of the shoulder blade (acromion). The joint between the clavicle and acromion (AC joint) is reinforced with several ligaments (acromioclavicular ligaments and coracoclavicular ligaments).
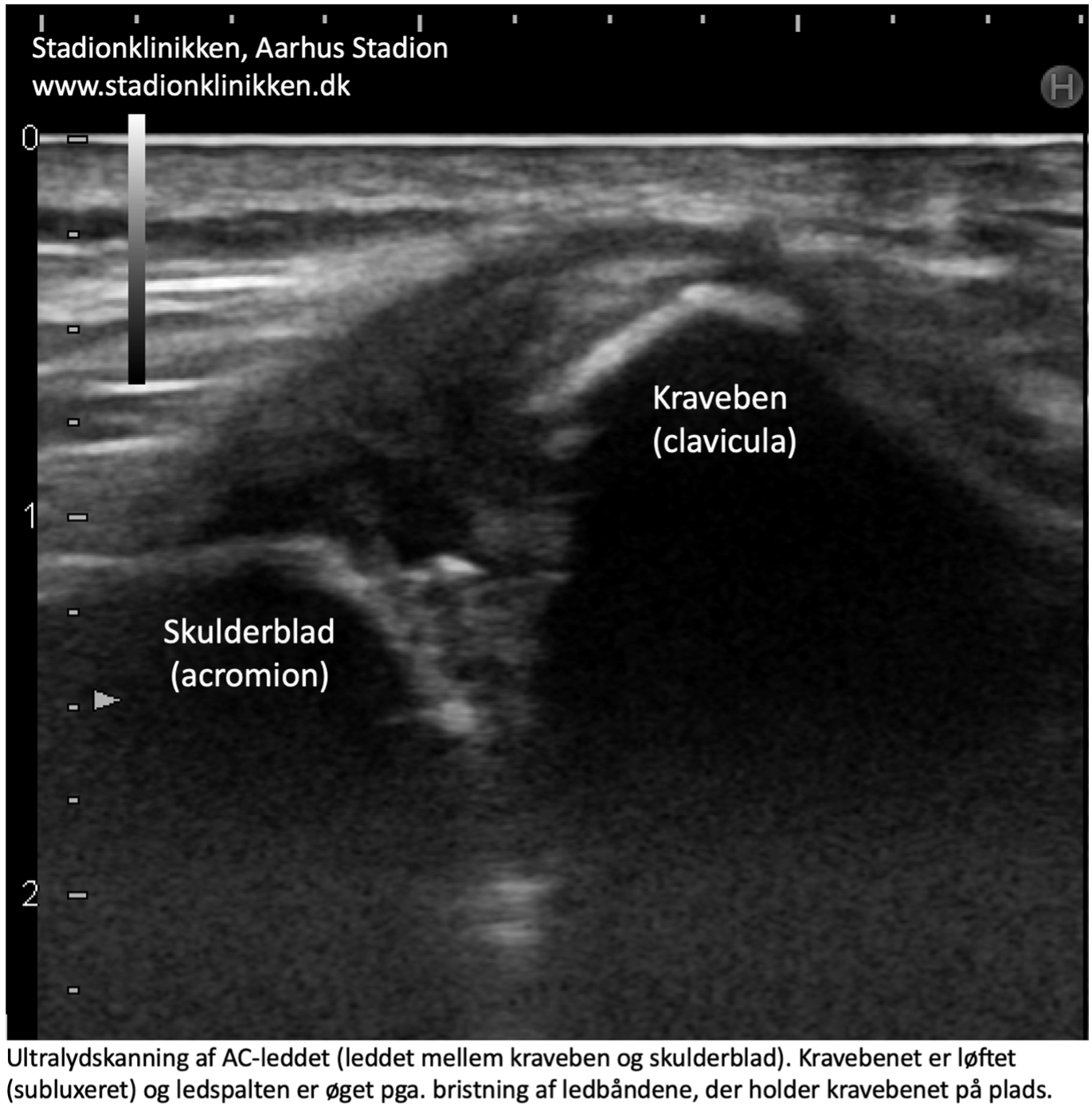
The joint between shoulder blade and collarbone

A. Clavicula (Collarbone)
B. Lig. transversum scapulae
C. Scapula (Shulder blade)
D. Acromion
E. Ligamentum acromioclaviculare
F. Ligamentum coraco-acromiale
G. Lig. Trapezoideum (Lig. coracoclaviculare)
H. Lig. conoideum (Lig. coracoclaviculare)
{kind=link}