Anatomy
On the outside of the outer femoral prominence (greater trochanter), many muscles attach to the buttocks and around the hip. Between the various muscle tendon attachments are mucosal sacs to reduce the strain on muscles and tendons when they slide over the bony prominence or against each other.
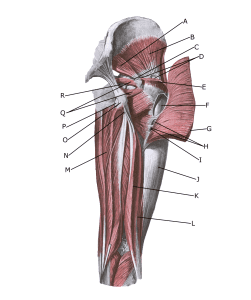 The gluteal muscles from behind:
The gluteal muscles from behind:
A. piriformis
B. gluteus minimus
C. Bursa m. piriformis
D. Bursae trochantericae m. glutei medii
E. gluteus medius (resectus)
F. Bursa trochanterica m. glutei maximi
G. gluteus maximus
H. Bursae intermusculares mm. gluteorum
I. Tuberositas glutea
J. Tractus iliotibialis
K. biceps femoris (caput longum)
L. biceps femoris (caput breve)
M. adductor magnus
N. subtendinea m. bicipitis femoris superior
O. Tuber ischiadicum
P. ischiadica m. glutei maximi
Q. gemilli sup. Et inf.
R. ischiadica m. obturatorii interni
{kind=link}