Anatomy
The lower leg consists of two bones: the tibia and fibula. The calf muscles are divided into 3 groups (muscle compartments) of strong muscle membranes (fascia) that are partially rigid: an anterior muscle compartment (comprising the flexor muscles of the foot, the extensors), an external (lateral) muscle compartment (comprising the peroneal muscles) and a posterior muscle compartment (comprising the extensor muscles of the foot, the flexors), which is divided into a superficial and a deep part.) Each muscle group has its own blood and nerve supply.
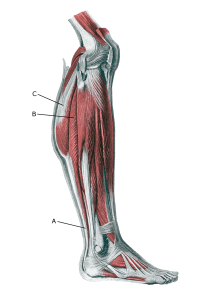
Lower leg:
A. Tendo calcaneus (Achillis)
B. M. soleus
C. M. gastrocnemius