Anatomy
The calf muscle (M. gastrocnemius) consists of two muscle heads that merge into a broad tendon which continues as the Achilles tendon. Attached to the front edge of the Achilles tendon is another of the large calf muscles (M. soleus), which thus forms part of the Achilles tendon. The Achilles tendon thus comprises the three calf muscles (Triceps Surae). The Achilles tendon attaches to the heel bone (calcaneus). Just in front of the Achilles tendon’s attachment to the heel bone is a bursa.
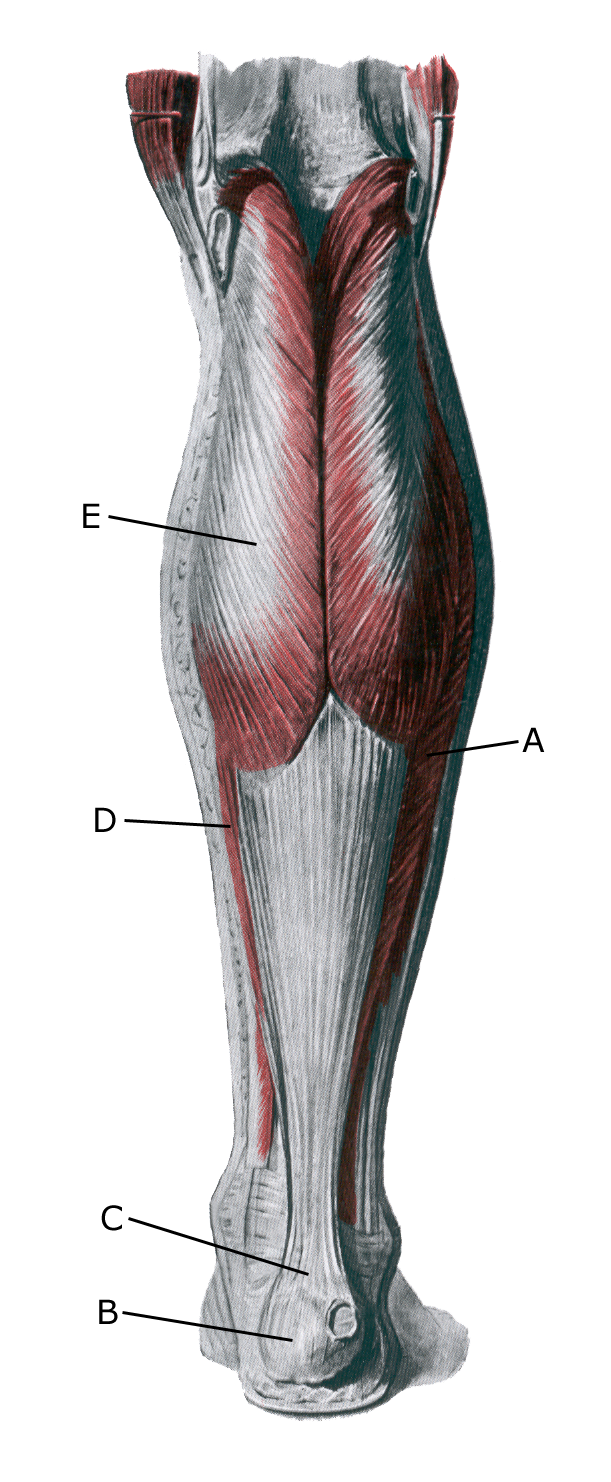 Lower leg from behind:
Lower leg from behind:
A. M. soleus
B. Tuber calcanei
C. Tendo calcaneus (Achillis)
D. M. gastrocnemius
Cause
“Inflammation” of the Achilles tendon is caused by repeated strain, often resulting from running and pushing off. The risk of strain injuries to the Achilles tendon increases with age. The vast majority of cases of inflammation (tendinitis) of the Achilles tendon are located 3–6 cm above the attachment to the heel bone and, less commonly, at the attachment to the heel bone (enthesitis), where it is often combined with inflammation of the bursa (bursitis).
These changes may be caused by degenerative changes in the tendon (tendinosis). In recent years, the condition has been referred to as Achilles tendinopathy, regardless of whether the cause is inflammation (tendinitis) or degeneration (tendinosis). Tendinopathy increases the risk of partial and complete ruptures.
Symptoms
Pain when the Achilles tendon is activated (during running and push-off), when pressure is applied to the tendon, and when the tendon is stretched. The tendon often feels thickened. In some cases, symptoms may persist for several years.
Examination
In cases of gradually developing tenderness or pain without sudden worsening, the diagnosis is made through a clinical examination. In cases of prolonged symptoms, lack of improvement with rest and rehabilitation, and in all instances where a snapping sensation or sudden shooting pain is felt in the tendon, the patient should be examined by a relevant specialist and undergo an ultrasound scan.
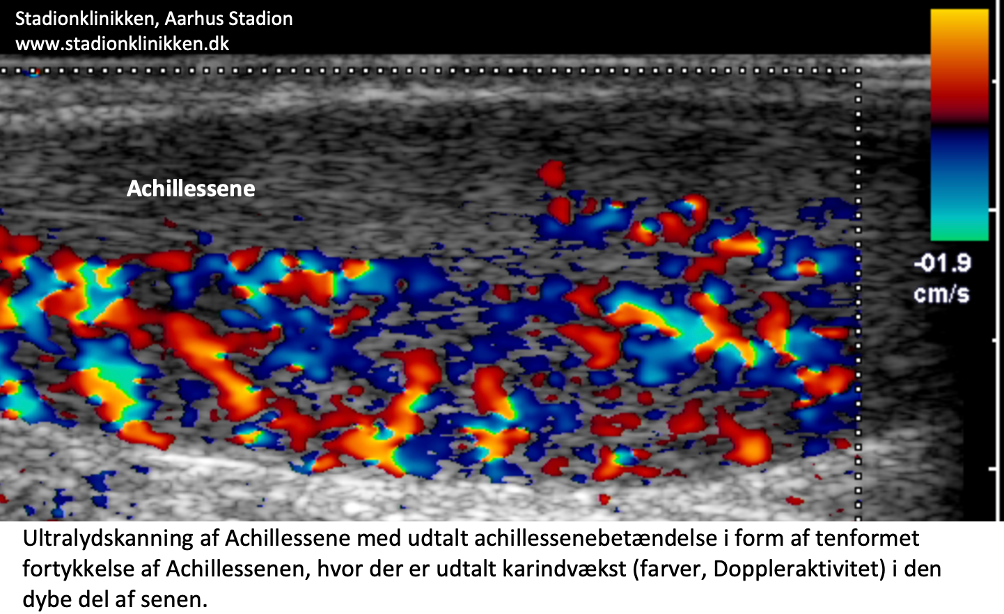
The ultrasound scan can, among other things, reveal the extent of changes in the tendon: tendon thickness, blood vessel ingrowth into the tendon (Doppler activity) – see ultrasound scan, inflammation of the tendon (tendinitis), degenerative changes in the tendon (tendinosis), calcifications in the tendon, inflammation of the tendon sheath (peritendinitis), inflammation of the bursa (bursitis) and (partial) tears.
{kind=link}
Treatment
Treatment for overuse Achilles tendinitis primarily involves resting from the activity causing the pain (running), stretching, and gradually increasing strength training within the pain threshold.
If treatment is started promptly, the injury may in some cases heal within a few weeks. If the pain has persisted for several months, and if an ultrasound scan reveals thickening of the Achilles tendon, a rehabilitation programme lasting several months or up to six months is often to be expected. Particular emphasis is placed on strength training by activating the tendon whilst it is being stretched (eccentric training) or slow, heavy strength training (Beyer R, et al. 2015).
If there is a lack of progress with rest and rehabilitation, it may be worth considering supplementing the rehabilitation with medical treatment in the form of anti-inflammatory tablets, NSAID or Corticosteroid –injections around the thickened part of the tendon.(Johannsen F, et al. 2018). As the administration of adrenal cortex hormones is always part of a long-term rehabilitation programme for a serious, chronic injury, it is essential that the rehabilitation programme lasts for (at least) six months in order to reduce the risk of relapse and tears.
Senen kan naturligvis ikke efter en langvarig skadesperiode holde til maksimal belastning efter kun en kortvarig genoptræningsperiode. Et halvt års genoptræning inden maksimal belastning (spring, spurter) tillades, er ikke usædvanlig. Se Generelt, kronisk senebetændelse.
Bandage
Taping for Achilles tendon problems is of questionable benefit, but it is worth a try. See tape
Complications
If the condition does not improve steadily, a (further) ultrasound scan should be carried out to rule out a (partial) rupture of the Achilles tendon.
Few sports injuries carry such a high risk of causing chronic, sports-limiting symptoms as Achilles tendinitis. In the most severe cases, despite all attempts at treatment and rehabilitation, the injury will often result in the athlete having to give up sport.
In particular
As Achilles tendinitis is difficult to treat, it is vital to prevent the injury from recurring. The principles of rehabilitation (Rehabilitation, generel) should be followed to avoid a rapid increase in training load at the start of the season, following periods of injury, or when using new running shoes.
Ultrasound scans of asymptomatic athletes frequently reveal changes in the Achilles tendon that have been shown to increase the risk of developing symptoms of Achilles tendinitis over the next 12 months (Fredberg U, et al. 2008). Preventive strength and flexibility training can therefore should be started before the injury causes symptoms.
Rehabilitation
Rehabilitation program
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.