Anatomy
 The shoulder joint consists of the humeral head of the humerus (caput humeri) and the articular surface of the scapula (cavitas glenoidalis). A meniscus (labrum glenoidale) runs all the way around the edge of the shoulder blade’s articular surface.The joint is surrounded by a joint capsule that is reinforced by several ligaments. Surrounding the joint capsule are the shoulder muscles that further reinforce the joint.
The shoulder joint consists of the humeral head of the humerus (caput humeri) and the articular surface of the scapula (cavitas glenoidalis). A meniscus (labrum glenoidale) runs all the way around the edge of the shoulder blade’s articular surface.The joint is surrounded by a joint capsule that is reinforced by several ligaments. Surrounding the joint capsule are the shoulder muscles that further reinforce the joint.
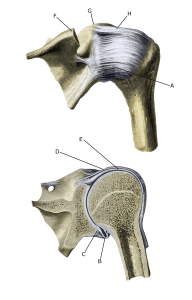
Shoulder joint:
A. Capsula articularis
B. Capsula articularis
C. Labrum glenoidale
D. Capsula articularis
E. biceps brachii (caput longum)
F. Acromion
G. Processus coracoideus
H. Ligamentum coracohumerale