Anatomy
 The elbow joint is the joint connection between the humerus and the two bones of the forearm: the radius and the ulna. Several ligaments reinforce the elbow joint: the medial collateral ligament, the lateral collateral ligament and the anular radius ligament (which goes around the head of the radius). Many of the forearm muscles that bend the wrist backwards and stretch the fingers attach to the outer bony projection of the humerus on the elbow (epicondylus lateralis).
The elbow joint is the joint connection between the humerus and the two bones of the forearm: the radius and the ulna. Several ligaments reinforce the elbow joint: the medial collateral ligament, the lateral collateral ligament and the anular radius ligament (which goes around the head of the radius). Many of the forearm muscles that bend the wrist backwards and stretch the fingers attach to the outer bony projection of the humerus on the elbow (epicondylus lateralis).
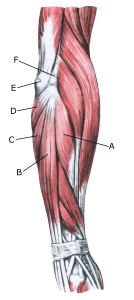
Forearm extensors:
A. M. extensor carpi radialis brevis
B. M. extensor digitorum
C. M. extensor carpi ulnaris
D. M. anconeus
E. Olecranon (Tip of the elbow)
F. Epicondylus lateralis
Cause
Pain at the tendon attachment on the outside of the elbow is very common, affecting 1-3% of the population annually.
With repeated, consistent (over)loading, the strength of the muscle attachment is exceeded. This causes microscopic tears in the tendon and especially at the tendon attachment on the outside of the elbow (enthesitis), resulting in ‘inflammation’.
Tendonitis is a warning sign that the training is too strenuous for the muscle tendon, and if the load is not reduced, a chronic ‘inflammation’ can develop that is difficult to treat. The condition is also known as ‘tennis elbow’ and in the world of sport is often a result of incorrect hitting technique or inappropriate equipment (racket).
Using a new, heavier racket, heavier balls or stiffer stringing can contribute to the condition. The one-handed backhand stroke in particular causes the symptoms, as ball contact causes a very strong strain on the muscle attachments on the outside of the elbow (extensor tendons).
The backswing of the backhand before the stroke or the braking of the forehand stroke can also be a contributing factor, as this also places a heavy load on the tendon attachment of the same muscle group on the outside of the elbow.
Women, smokers, people with high cholesterol or manual labour have a significantly increased risk of developing tennis elbow (Chen Q. et al., 2024).
Symptoms
Tenderness and pain on the bony prominence on the outside of the elbow (epicondylus lateralis) with aggravation when bending the wrist backwards (extension) against resistance and when stretching. In some cases, the pain is localised slightly below the tendon attachment.
Symptoms usually subside with relief, but can last for several years. In rare cases, partial or total rupture of the tendon attachment can occur, causing a sudden pop with worsening pain.
Examination
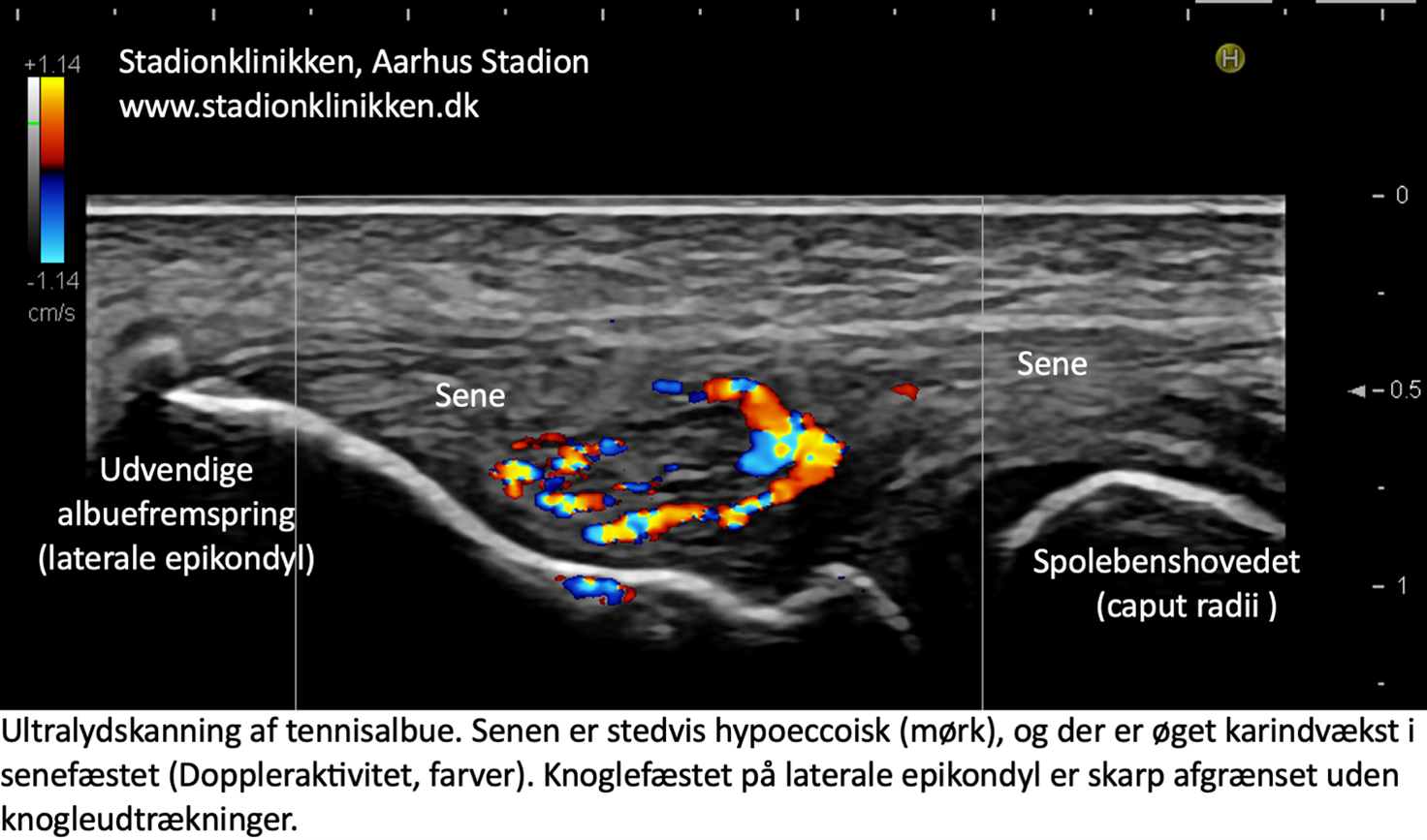{kind=link}
Treatment
Early correction of the triggering cause (load, impact technique and equipment adaptation) is crucial to the outcome of rehabilitation. The recommended treatment is relief from pain-inducing activity, stretching and slowly increasing strength training of the forearm muscles within the pain threshold.
If you take a break from or reduce the amount of the triggering activity, the symptoms disappear spontaneously in weeks to months for most people, but it is not uncommon for the discomfort to last for years, which is why exercise correction is important as soon as the first symptoms start.
Relapses are frequent, especially if the triggering cause has not been eliminated (lack of strength, incorrect technique). If the discomfort does not subside with load reduction and careful rehabilitation within the pain threshold and pain is the main problem, rehabilitation can be supplemented with medical treatment in the form of adrenal cortex hormone.
Adrenal cortex hormone injection for tennis elbow symptoms has a well-documented short-term effect, but has no documented long-term effect, possibly due to relapse conditioned by a forced increase in exercise intensity when the pain is reduced (Krogh TP, et al. 2013). However, this does not affect the results of any subsequent surgery (Ha C, et al. 2023).
Only correction/reduction of the triggering cause(s) and slow rehabilitation within the pain threshold have a long-term effect (Couppé C, et al. 2022). If there is no improvement, surgery can be considered, but the results are not well documented.
Bandage
Some people find that applying tape (or a bandage) around the forearm just below the elbow improves symptoms, see tape, but this treatment is also undocumented.Wrist and elbow bandages can provide relief, but there is a lack of evidence of effectiveness.
Complications
If no progress is made, you should reconsider whether the diagnosis is correct or if complications have arisen.
In particular, the following should be considered:
- Inflammation of the bursa at the elbow
- Rheumatoid arthritis in the elbow joint
- Ligament ruptures on the outside of the elbow
- Pinching of the radial nerve
- Thrower’s elbow (discomfort triggered from the elbow joint itself and joint capsule and possibly from the ulnar nerve)
- Muscle rupture