Anatomy
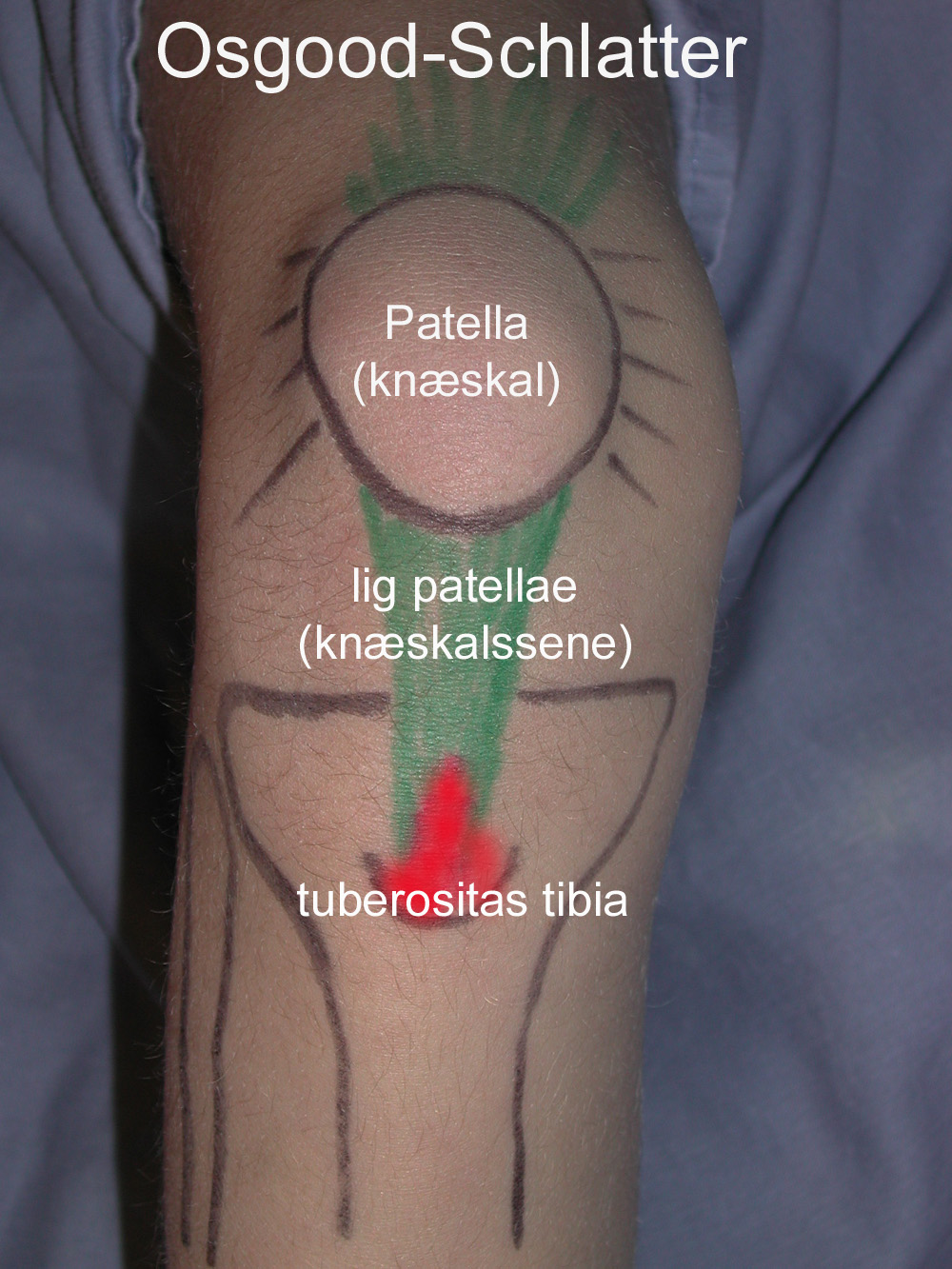
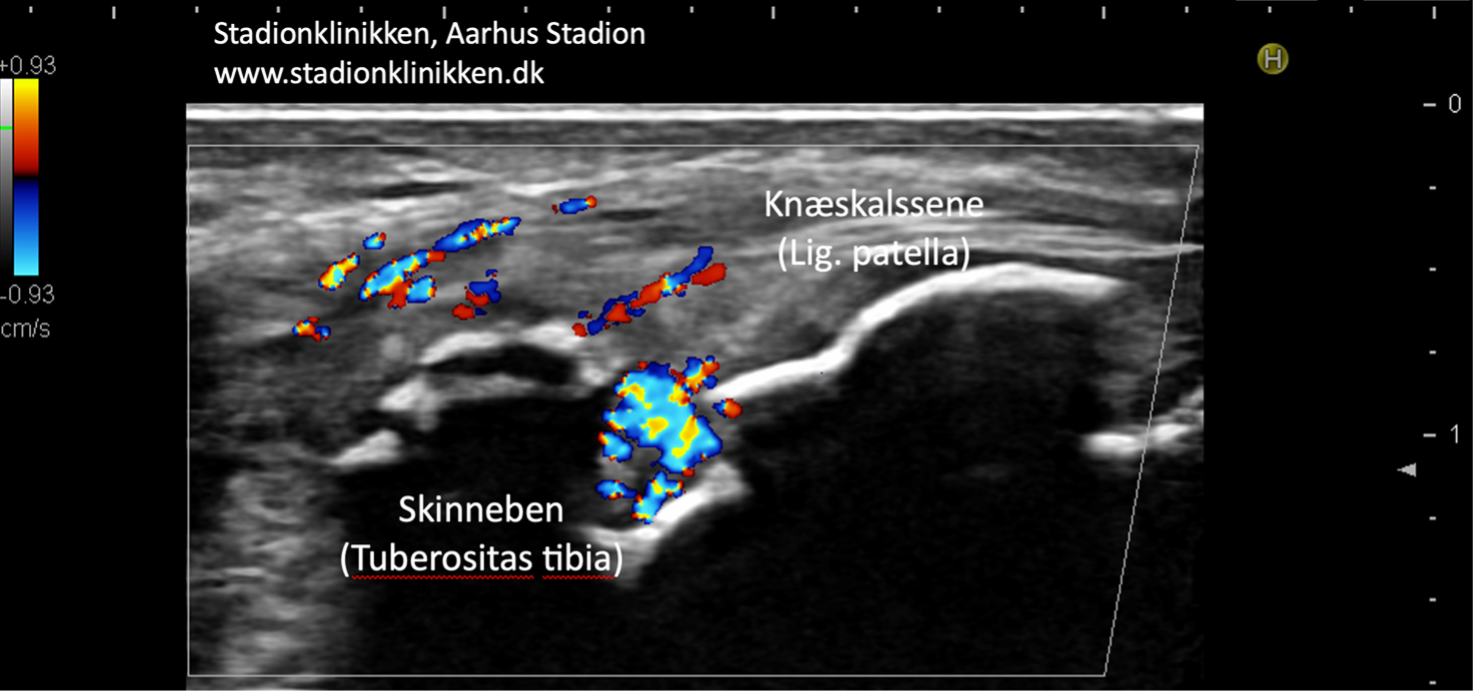
The large anterior thigh muscle (musculus quadriceps femoris) consists of four muscles (m vastus lateralis, m vastus medialis, m vastus intermedius and m rectus femoris). The muscles all attach to the top edge of the kneecap. The patella tendon (ligamentum patellae) connects the lower edge of the patella to the upper, anterior part of the tibia (tuberositas tibiae).
The function of the patellar tendon is to transmit the force exerted by the large anterior thigh muscle when the knee is extended. Where the patellar tendon attaches to the patella and tibia, in adolescents there is a growth zone (apophysis).
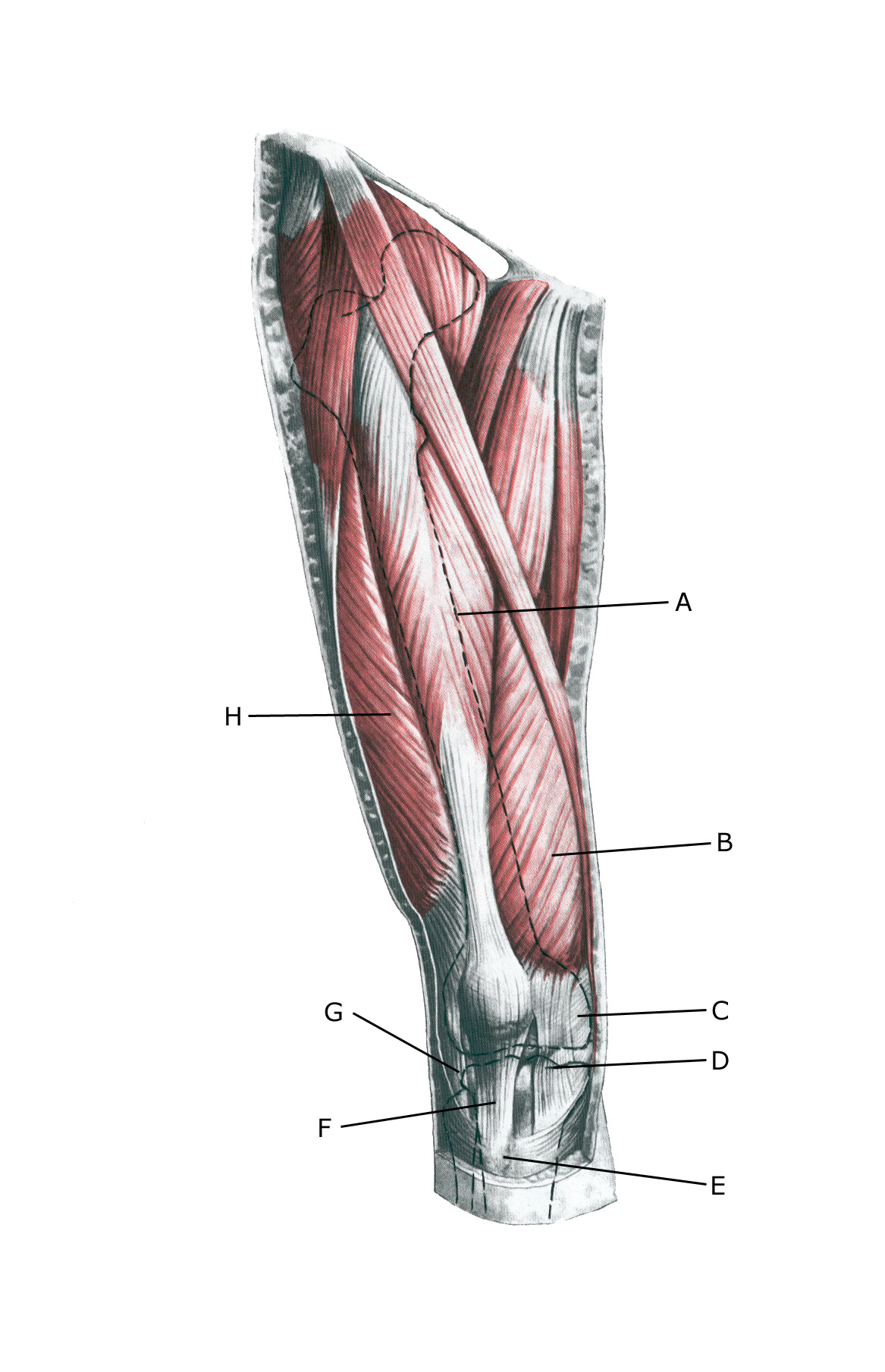 Knee from the front:
Knee from the front:
A. M. rectus femoris
B. M. vastus medialis
C. Retinaculum patellae mediale
D. Retinaculum patellae mediale
E. Tuberositas tibiae
F. Lig. Patellae
G. Retinaculum patellae laterale
H. M. vastus lateralis
{kind=link}
{kind=link}