Anatomy
The spine is made up of box-shaped vertebrae that are held in place partly by the shape of the bones, partly by ligaments and partly by the large and small back and abdominal muscles. Interspersed between the vertebrae are cartilage discs (disci) that act as shock absorbers. The discs are close to the spinal canal, from which nerves run to the legs.
Back vertebrae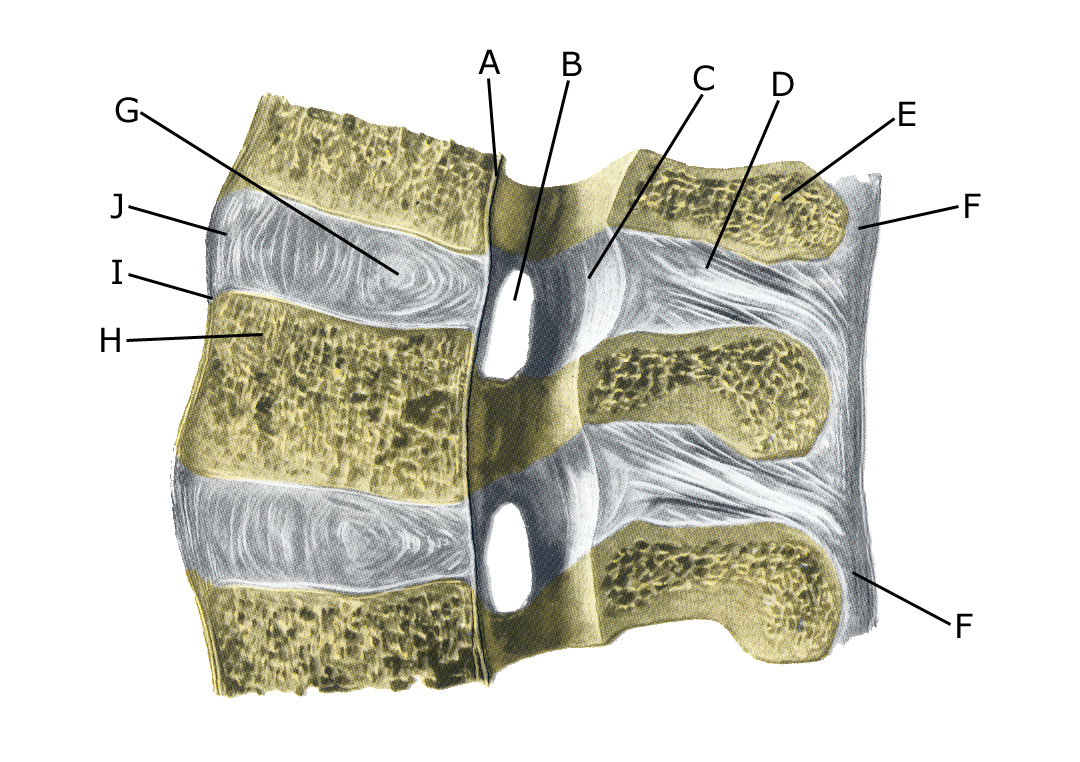
A. Ligamentum longitudinale posteriu
B. Foramen intervertebrale
C. Ligamentum flavum
D. Ligamentum interspinale
E. Processus spinosus
F. Ligamentum supraspinale
G. Nucleus pulposus
H. Corpus vertebrae
I. Ligamentum longitudinale anterius
J. Discus intervertebralis