Anatomy
The muscles and tendons around the ankle joint are divided into 3 groups. A group at the front of the ankle (extensor tendons) that bend the foot up, a group behind the inside of the ankle (long flexor tendons) and a group behind the outside of the ankle (peroneal tendons) that help to stabilise and stretch the ankle. The tendons are partially embedded in tendon sheaths.
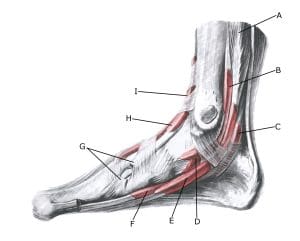
Foot, inner
A. M. flexor digitorum longus
B. Vagina synovialis tendinis m. tibialis posterioris
C. Vagina synovialis tendinis m. flexoris hallucis longi
D. Vagina tendinum m. flexoris digitorum pedis longi
E. Tendo m. tibialis anterioris
F. Vagina tendinis m. tibialis anterioris
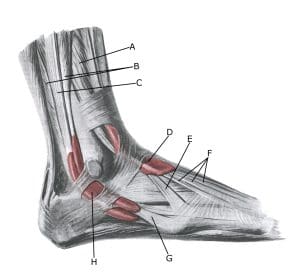 Foot, outer
Foot, outer
A. M. extensor digitorum longus
B. M. peroneus brevis
C. M. peroneus longus
D. Vagina tendinum m. extensoris digitorum pedis longi
E. M. peroneus tertius
F. Tendines m. extensoris digitorum longi
G. Vagina synovilis mm. peroneorum communis
{kind=link}