Anatomy
The ankle joint is stabilised by a joint capsule, which is reinforced on the inside (medially) by a broad, fan-shaped ligament (lig. deltoideum), and on the outside (laterally) by three ligaments: an anterior one (lig. talofibulare anterius, ATFL), a middle one (lig. calcaneofibulare) and a posterior one (lig. talofibulare posterius). The ligaments stabilise the ankle joint, particularly during twisting, running with changes of direction, etc. The tibia and fibula are held together in the ankle joint by, amongst other things, two ligaments (lig. tibiofibulare anterius and posterius).
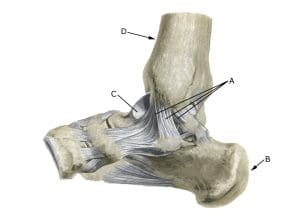
Ankle joint inside
A. Medial deltoid ligament
B. Calcaneus (heel bone)
C. Talus
D. Tibia (shin bone)
Cause
Rupture of the medial collateral ligaments of the ankle joint is much rarer than rupture of the lateral collateral ligaments of the ankle joint. Rupture of the medial collateral ligaments of the ankle joint occurs when the foot wiggles (pronation), causing the medial ligaments to overstretch and rupture. In mild cases it is called a sprain/strain and in severe cases a full or partial rupture/tear.
There are often secondary injuries associated with ligament ruptures, including rupture of the ligaments that hold the tibia and fibula together: syndesmosis rupture, fluid accumulation in the joint (traumatic synovitis) and tendonitis, rupture of the metatarsal ligaments, ankle fracture, cartilage damage in the ankle joint.
In some cases, ankle ligament ruptures are complicated by inflammation of the joint capsule around the ankle joint (capsulitis).
Symptoms
Pain on and below the medial malleolus, swelling due to bleeding, and pain when walking.
Examination
Diagnosis is made on clinical examination, where in mild cases (sprains) there is only swelling and no discomfort with normal walking, but usually pressure tenderness at the attachment of the internal ligaments to the inner ankle bone. The amount of swelling is not a measure of the extent of the injury.
Pronounced swelling and pain should be examined by an appropriate professional to rule out ankle fractures and ruptured ligaments between the tibia and fibula. If a fracture or syndesmosis rupture is suspected, an X-ray of the ankle joint should be performed. The Ottawa ankle rule provides guidance on when an X-ray should be taken (Yolanda E Gomes et al 2022).
Previous vigorous twisting of the ankle joint in the acute stage to assess the degree of looseness is no longer indicated as this does not affect the choice of treatment.
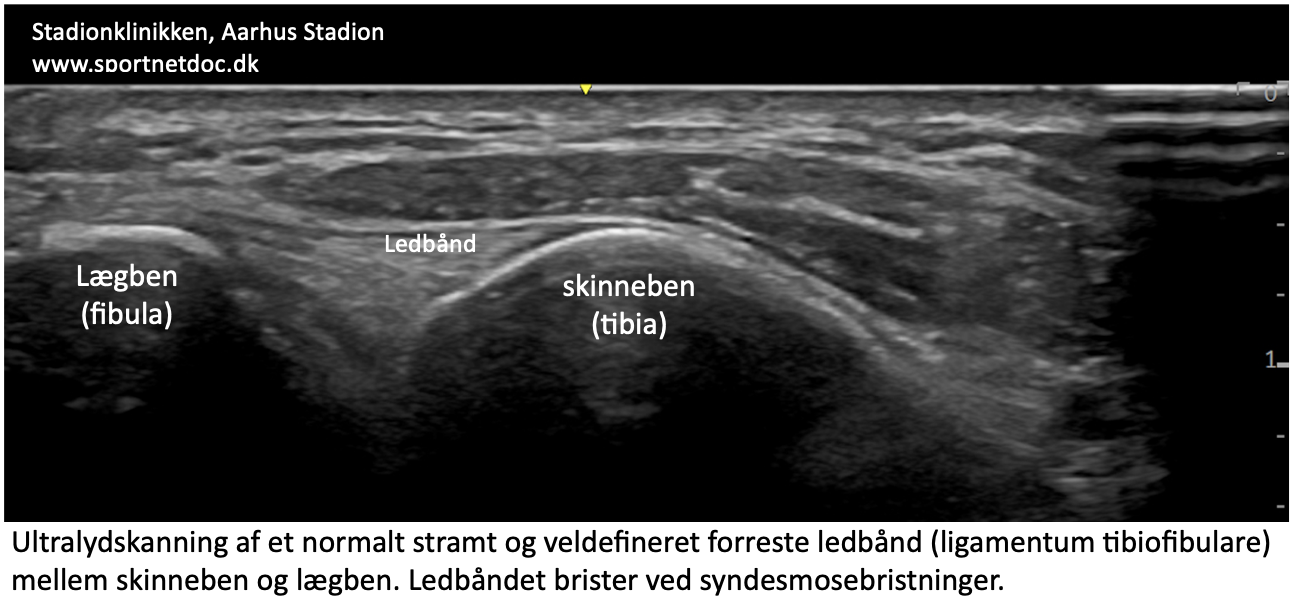
Ultrasound scanning can produce internal ligaments – see ultrasound scan here and tibiofibular ligaments (lig. tibiofibulare ant. inf.) that rupture in syndesmosis rupture, see ultrasound scan here and inflammation in capsulitis (Colò G, et al. 2023). Ultrasound scanning is suitable for seeing small bone tears at the ligament attachments.
{kind=link}
{kind=link}
Dynamic ultrasound scanning can assess ligament looseness (the ligament is stressed during simultaneous ultrasound scanning to see if the joint gap increases as a sign of ligament rupture) (Heitz PH, et al. 2023).
Treatment
The treatment of ligament injuries today is conservative (rehabilitation) (Loozen L, Veljkovic A, Younger A. 2023). In the past, many patients underwent surgery and bandaging, which has largely been abandoned for uncomplicated ligament ruptures. In cases of repeated ankle sprains, syndesmosis tears with significant looseness, and complex injuries (fractures, multiple torn ligaments), surgery is often indicated (Corte-Real N, Caetano J. 2021).
Bandage
During the rehabilitation process, the use of tape is recommended when running on uneven surfaces or running with rapid changes of direction is initiated. The ligaments contain nerve cells (proprioreceptors) that send information to the brain about the position of the ankle joint. From the brain, information is sent to the muscles, which are activated to keep the ankle joint in the correct position. When the ligaments are damaged, these nerve pathways don’t function optimally and the risk of twisting the foot again increases.
The function of the tape is primarily to stimulate the small nerve cells (proprioreceptors) in the skin so that they can ‘substitute’ for the temporarily damaged nerve cells in the ligaments. The function of the tape is thus not a purely mechanical ‘stabilisation’ of the ankle joint, Tape-5. In some cases, certain types of bandages around the ankle joint can be beneficial for 5-6 weeks.
Specialised bandages have been shown in some studies to reduce the risk of ligament re-injury.
Complications
If the progress is not smooth, you should consider whether the diagnosis is correct or if complications have arisen:
In particular, the following should be considered:
- Rupture of ligaments between the tibia and fibula
- Periosteal avulsions
- Tendon synovitis
- Concentration of fluid in the joint (traumatic synovitis)
- joint cartilage damage, osteoarthritis (osteochondral lesion)
If rehabilitation is approached sensibly, it is rare for the injury to result in a chronically loose ankle joint. If a chronically loose ankle joint does develop, intensive balance training is recommended. Neglecting treatment may lead to the development of flat feet.
If rehabilitation is not sufficient, bandages may be tried. If this is also not sufficient, surgery to tighten the ligaments may be attempted (Corte-Real N, Caetano J. 2021).
In particular
Tilt board exercises (see exercise 1 and exercise 2) are important in both rehabilitation and prevention (Al Attar WSA, et al. 2022).
{kind=link}
{kind=link}
If you have a history of ligament injuries in the ankle joint, seesaw exercises should be performed regularly for the rest of your active sports career as a preventative measure. Start by standing on both legs on the seesaw and support with your hands on the wall. Gradually release the support with your hands and finally train with support on one leg only. You can brush your teeth morning and evening on the seesaw.