Anatomy
The bones of the knee joint include the femur (thigh bone), tibia (shin bone) and patella (kneecap). The articular surfaces of the femur, tibia and patella are covered by a layer of cartilage a few millimetres thick, which serves to reduce the load on the articular surfaces. Both inside and outside the joint there is a ring-shaped disc of cartilage (meniscus). The knee joint is reinforced by a joint capsule, which is reinforced at the sides by an outer and inner collateral ligament (lateral and medial collateral ligaments). The inner meniscus is attached to the inner collateral ligament, whilst the outer meniscus is not attached to the outer collateral ligament.
Knee joint from the front:
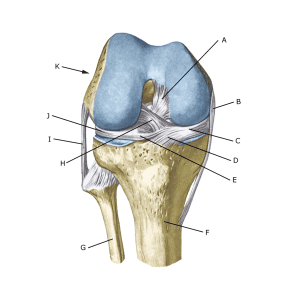
A. Ligamentum cruciatum posterius (Posterior cruciate ligament)
B. Ligamentum collaterale mediale/tibiale (Inner collateral ligament
C. Meniscus medialis (Inner meniscus)
D. Insertio anterior menisci medialis
E. Ligamentum transversum genus
F. Tibiae
G. Fibulae
H. Ligamentum cruciatum anterius (Anterior cruciate ligament)
I. Ligamentum collaterale laterale/fibulare (External collateral ligaments)
J. Meniscus lateralis (Outer meniscus)
K. Femur
Knee joints from above:
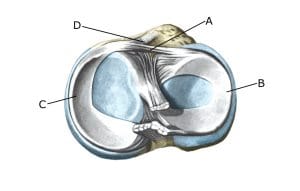
A. Ligamentum transversum genus
B. Meniscus lateralis (Outer meniscus)
C. Meniscus medialis (Inner meniscus)
D. Insertio anterior menisci
{kind=link}