Anatomy
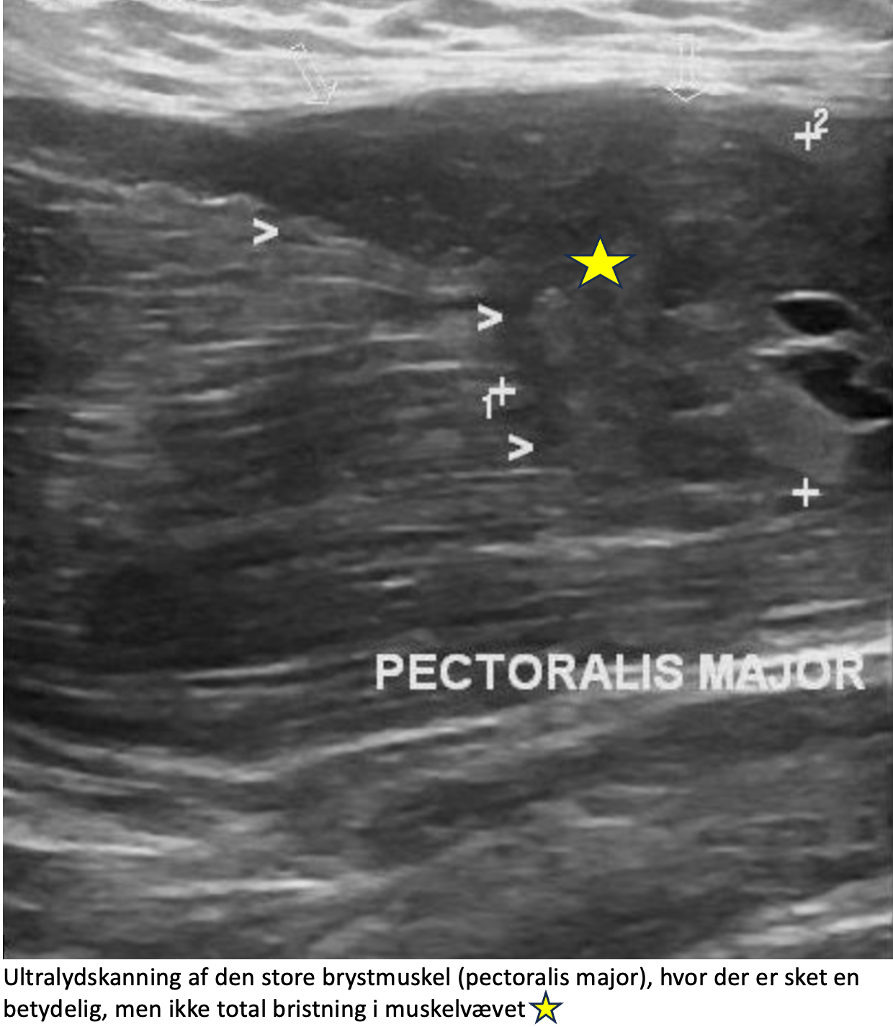
The pectoralis major muscle (M pectoralis major) is fan-shaped and covers the front of the chest wall and attaches to the humerus (crista tuberculi majoris). The function of the pectoralis major is, among other things, to bring the arm towards the body and to flex and internally rotate the shoulder (as in throwing). The large pectoral muscle forms the anterior fold of the armpit (anterior axillary fold).
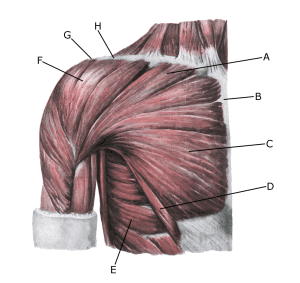
Shoulder and upper arm muscles, front view:
A. M. pectoralis majo
B. Sternum
C. M. pectoralis major
D. M. pectoralis major
E. M. serratus anterior
F. M. deltoideus
G. Acromion
H. Clavicula
{kind=link}