Anatomy
The elbow joint is the joint connection between the humerus and the two bones of the forearm: the radius and ulna. The three major nerves: radial, ulnar and median can all be pressurised around the elbow. The ulnar nerve is located in a canal (sulcus ulnaris) behind the inner elbow prominence (medial epicondyle), where it is covered in one area by a fibrous layer (fascia) (cubital tunnel).
Cause
Repeated bending and stretching of the elbow (e.g. weight lifting, tennis) can cause damage to the ulnar nerve.One of the most common places where the nerve can become pinched/irritated is around the elbow, where the ulnar nerve can be injured in several ways.The nerve can be pinched in the sulcus ulnaris, where the nerve can be pinched by the fibrous coating that holds the nerve in place in the canal (cubital tunnel syndrome).
The nerve can also be pinched in a muscle channel 3-4 cm below the elbow on the forearm. If the nerve and possibly the inner head of the triceps muscle (which extends the elbow) can slip over the inner elbow projection (medial epicondyle) when the elbow is flexed and extended, this can also trigger symptoms from the nerve (snapping elbow) (Xarchas KC, et al. 2007).
Symptoms
A visible and often audible rubbing sensation on the inside of the elbow is triggered when the elbow is bent and stretched. There may be shock-like pain, tingling, pins and needles and possibly numbness and sleeping sensation down the inside of the forearm and on the little finger side of the hand corresponding to the nerve supply area. In severe cases, there may be reduced muscle strength in the thumb and little finger.
Examination
The diagnosis is usually made during a general clinical examination. Symptoms can often be provoked by tapping with a finger on the nerve behind the inner elbow prominence (Tinel’s sign). The discomfort can be induced by bending and stretching the elbow.
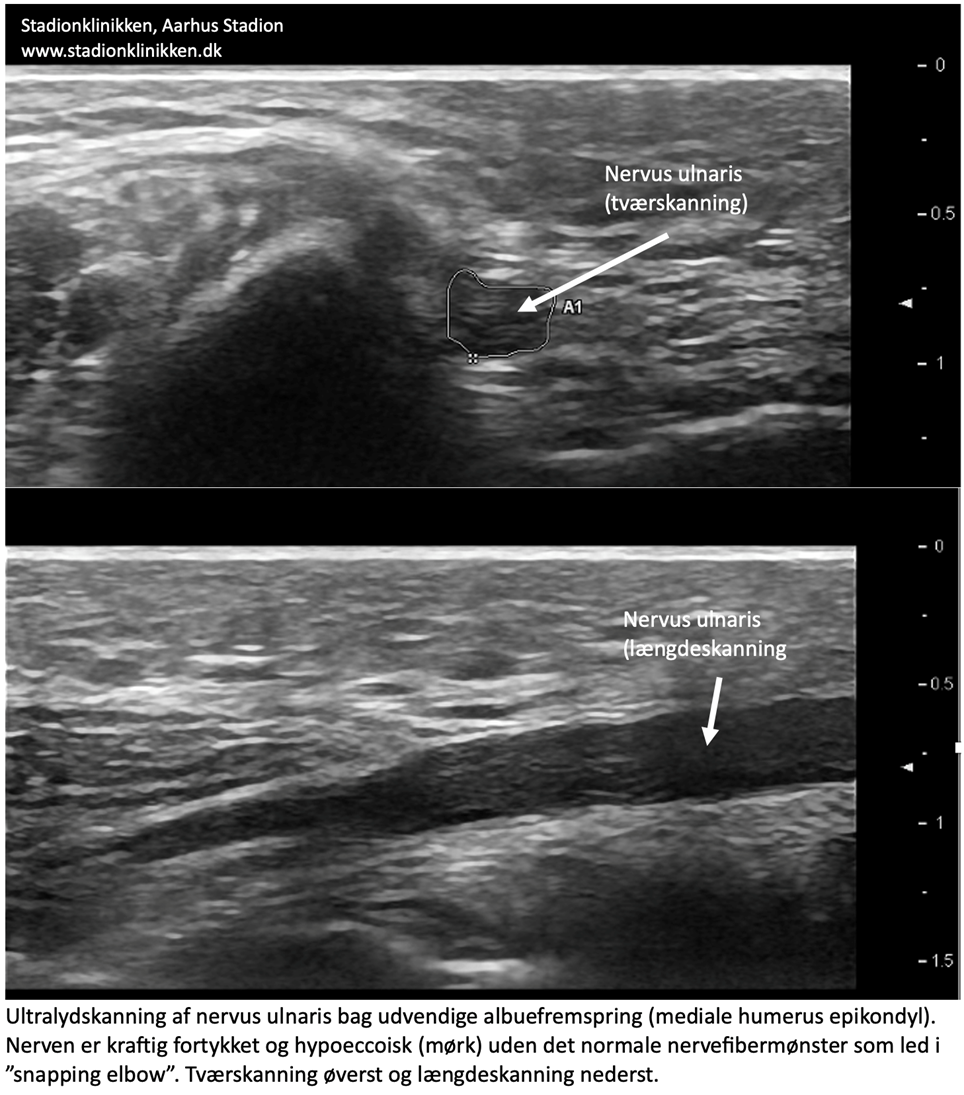
If there is any doubt about the diagnosis, an ultrasound scan can be performed where the ulnar nerve can be seen slipping out of the canal (sulcus ulnaris) and back and forth over the inner elbow protrusion when the elbow is flexed and extended.
Ultrasound scan video of “snapping elbow”
In some cases, the ulnar nerve is thickened. Impaired nerve function can be measured by nerve conduction studies, which are often normal if the nerve is only pinched or irritated periodically.
View ultrasound scan of the ulnar nerve behind the external elbow prominence.
{kind=link}
Treatment
Reducing the cause of the pain (loading, bending and stretching of the elbow, correction of striking technique, adaptation of equipment) is of course crucial to the outcome of rehabilitation. Rehabilitation also includes stretching and slowly increasing maintenance training within the pain threshold including the arm muscles.
If the discomfort does not subside with relief and gentle rehabilitation, surgery to stabilise the nerve in the canal (sulcus ulnaris) may be considered (Bjerre JJ, et al. 2018).
Bandage
Some people find that taping (or bandaging) the forearm just below the elbow improves symptoms, but this treatment is also unproven. Wrist and elbow bandages can provide relief, but there is a lack of evidence of effectiveness.
Complications
If no progress is made, you should reconsider whether the diagnosis is correct or if complications have arisen.
In particular, the following should be considered:
- Inflammation of the bursa at the elbow
- Rheumatoid arthritis in the elbow joint
- Ligament ruptures on the inside of the elbow
- Damage to the ulnar and median nerves
- Thrower’s elbow (discomfort triggered from the elbow joint itself and joint capsule)
- Muscle rupture