Anatomy
 but attaches to the little toe and big toe side of the foot. The plantar tendon is shock-absorbing and helps maintain the longitudinal arch of the foot.
but attaches to the little toe and big toe side of the foot. The plantar tendon is shock-absorbing and helps maintain the longitudinal arch of the foot. A. Aponeurosis plantaris
B. Tuber calcanei
{kind=link}
Cause
Overuse Inflammation’ of the Achilles tendon is a common cause of pain under the heel and is caused by repeated overloads such as running and pushing off. As the Achilles tendon is a functional extension of the Achilles tendon, the triggering stresses that lead to overuse injuries in the arch tendon and Achilles tendon are often the same. Flat feet, high insteps and being overweight predispose to Achilles tendonitis.
In rare cases, a sudden heavy strain can cause a partial/total rupture of the calcaneal tendon. Prolonged strain on the calcaneal tendon attachment can often result in a small bone pull-out (spur formation) in the calcaneal attachment.
This has given rise to the term ‘calcaneal tendonitis’, even though the spur formation is asymptomatic and insignificant, as the symptoms come from the thickened calcaneal tendon.
Symptoms
Slow-onset pain when running and taking off. The pain is usually localised directly under the heel, slightly inside (medial), but can extend into the arch. Difficulty starting with pain under the heel, for example in the morning.
There is often tenderness when pressure is applied to the calcaneal tendon attachment on the heel bone. The pressure pain can extend into the arch. When the hollow foot tendon ruptures, which most often occurs in the arch, there is acute severe pain in the arch, where it can be blood-drawing.
Examination
The diagnosis is usually made on clinical examination alone, where there is a slow onset of pain under the heel at the attachment of the hollow foot tendon. There is tenderness on pressure in the same place where the known pain can be triggered. Often the tenderness extends slightly into the arch. In all cases where a pop or sudden shooting pain is felt in the hollow foot tendon, you should be examined by an appropriate professional to rule out a (partial or total) fracture.
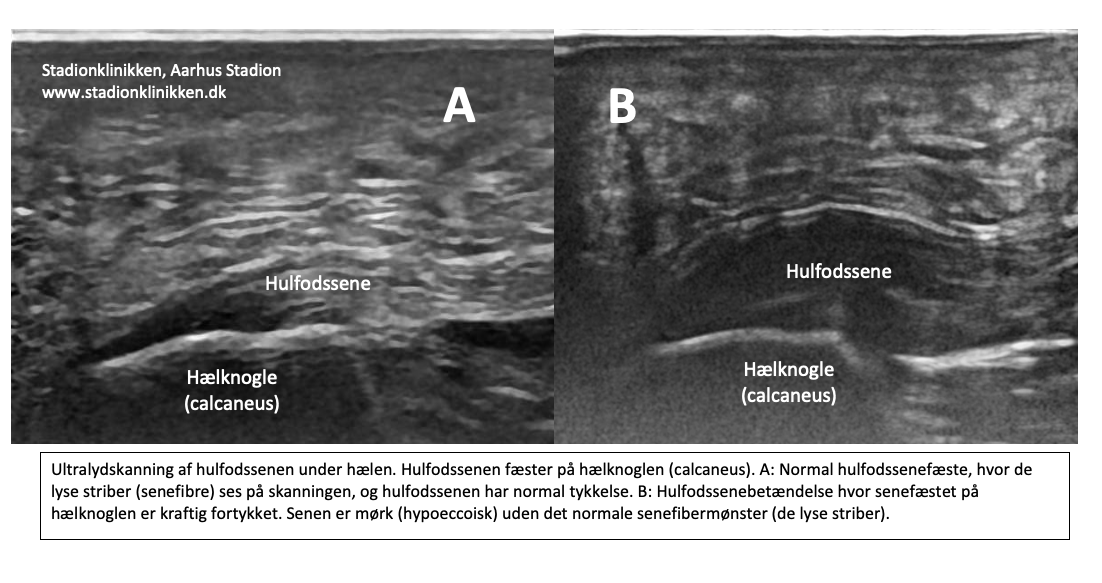
This is best determined by ultrasound and X-ray. In all cases where the progress is not smooth, an ultrasound scan will be useful to assess the extent of changes in the tendon: tendon inflammation (tendinitis), tendon scarring (tendinosis), tendon calcifications and (partial and total) ruptures. See ultrasound scan of the hollow foot tendon and ultrasound scanning can be used to monitor treatment (Johannsen F, Magnusson SP. et al. 2022).
{kind=link}
Treatment
The treatment of overuse tendinitis of the hindfoot consists primarily of relief from the pain-inducing activity (running, jumping), stretching and slowly increasing strength training within the pain threshold. If treatment is started quickly, the injury can sometimes heal in a matter of weeks.
If the pain has been present for several months and ultrasound scans show thickening and changes in the hollow foot tendon, a rehabilitation programme over several months/half years is often required. Particular emphasis is placed on strength training by activating the tendon while stretching it (eccentric training) or slow heavy strength training (Beyer R, et al. 2015 and Rathleff MS et al 2014).
If relief and rehabilitation are not successful, rehabilitation may be considered supplemented with medical treatment in the form of arthritis pills, NSAIDs or injection of adrenal cortex hormone around the thickened part of the tendon (Johannsen FE, et al. 2019) as part of a long-term rehabilitation programme over months (half a year). In some places, surgery is performed for plantar tendonitis if rehabilitation and medical treatment are not sufficient, although the evidence for the effect is modest (Johannsen F, et al. 2020).
Total ruptures of the subtalar tendon are treated as subtalar tendonitis with offloading for a few weeks, after which rehabilitation is started as described below. It often takes more than half a year before full sports activity can be resumed. In athletes with high demands on jumping power (e.g. gymnasts), surgery may be considered (Susanne Olesen Schaarup et al, 2020). After surgery, it can take up to 1 year before full sports activity can be resumed.
Bandage
Taping for hollow foot tendon problems is of questionable value, but can be tried. See taping
Complications
If progress is not smooth, you should reconsider possible differential diagnoses and complications.
In particular, the following should be considered:
- Partial or total rupture of the hollow foot tendon,
- Stress fracture in the foot
- Tendon synovitis
- If the hollow foot tendon is normal on ultrasound, Baxter’s nerve entrapment should be considered.
Additional imaging may often be necessary (X-rays and MRI scans).
Few sports injuries have such a high risk of causing chronic, athletically debilitating discomfort as hollow foot tendonitis. Long-term follow-up (5-15 years) has shown that a large proportion of patients continue to have fluctuating symptoms for many years (Hansen L, et al. 2018).
In particular
Running shoes should fit (tight heel cup) and have a good shock-absorbing effect. Shock-absorbing heel spur inserts with a cut-out corresponding to the sore area under the heel can be tried.
It is advisable to reduce running distances when changing shoes and increase distances slowly to avoid overuse injuries. It’s crucial to react to the first signs of soreness or pain so that training can be redirected before the condition develops into a chronic condition with the risk of having to stop sporting activity permanently.
Few sports injuries have such a high risk of causing chronic, athletically debilitating discomfort as hollow foot tendonitis. Long-term follow-up (5-15 years) has shown that a large proportion of patients continue to have fluctuating symptoms for many years.