Anatomy
The bones of the knee joint include the femur (thigh bone), tibia (shin bone) and patella (kneecap). There is also a small joint between the tibia and fibula (fibula). The knee joint is supported by a joint capsule, which is reinforced on the sides by an outer and inner collateral ligament (lateral collateral ligament (LCL) and medial collateral ligament (MCL)). Inside the knee there are two ligaments, the anterior and posterior cruciate ligaments (anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL)).
Knee joint from the front:
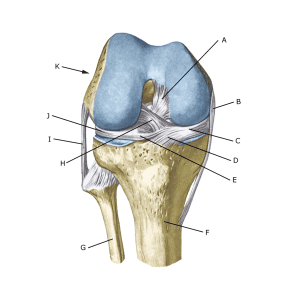
A. Ligamentum cruciatum posterius (Posterior cruciate ligament)
B. Ligamentum collaterale mediale/tibiale (Inner collateral ligament
C. Meniscus medialis (Inner meniscus)
D. Insertio anterior menisci medialis
E. Ligamentum transversum genus
F. Tibiae
G. Fibulae
H. Ligamentum cruciatum anterius (Anterior cruciate ligament)
I. Ligamentum collaterale laterale/fibulare (External collateral ligaments)
J. Meniscus lateralis (Outer meniscus)
K. Femur
 Lower leg on the outside:
Lower leg on the outside:
A. M. gastrocnemius
B. Caput fibulae
C. B. subtendinea m. bicipitis femoris inferior
D. M. biceps femoris (overcut)
E. Ligamentum collaterale laterale/fibulare (Unique lateral ligament)
F. M. plantaris
{kind=link}