Anatomy
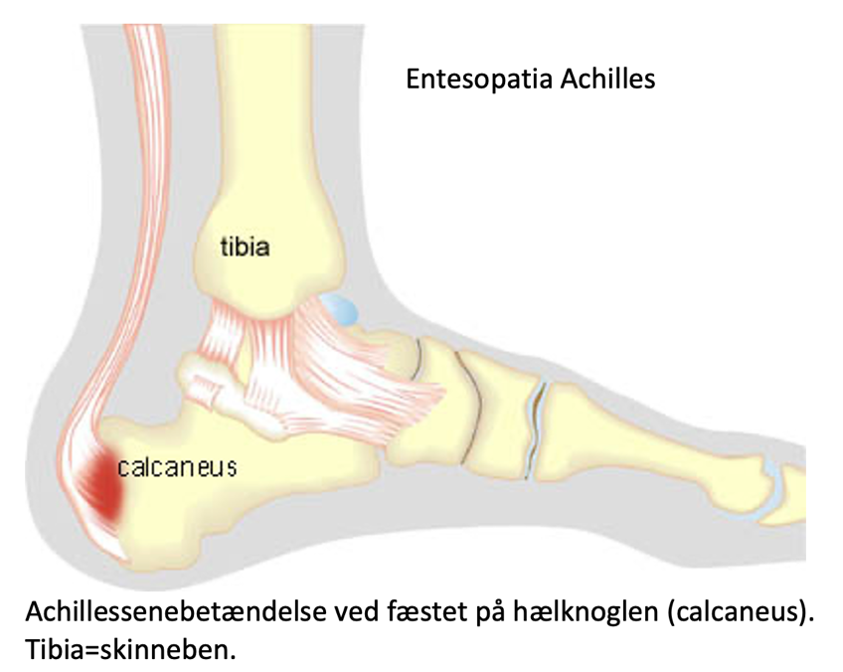
The calf muscle (M Gastrocnemicus) consists of two muscle heads that come together in a broad tendon band that continues into the Achilles tendon. Another large calf muscle (M Soleus) attaches to the front edge of the Achilles tendon and forms part of the Achilles tendon. The Achilles tendon attaches to the heel bone (calcaneus). The Achilles tendon thus consists of the 3 calf muscles (Triceps Surae). At the heel bone, there is a deep mucosal sac at the front (deep bursae tendinis Achilles) and a superficial mucosal sac at the back (superficial bursae subcutanea calcanei) of the Achilles tendon attachment. The bursae reduce the pressure on the Achilles tendon.
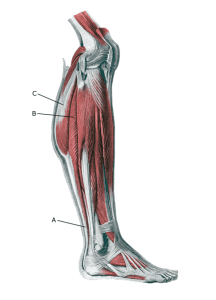
Lower leg:
A. Tendo calcaneus (Achillis)
B. M. soleus
C.M. gastrocnemius
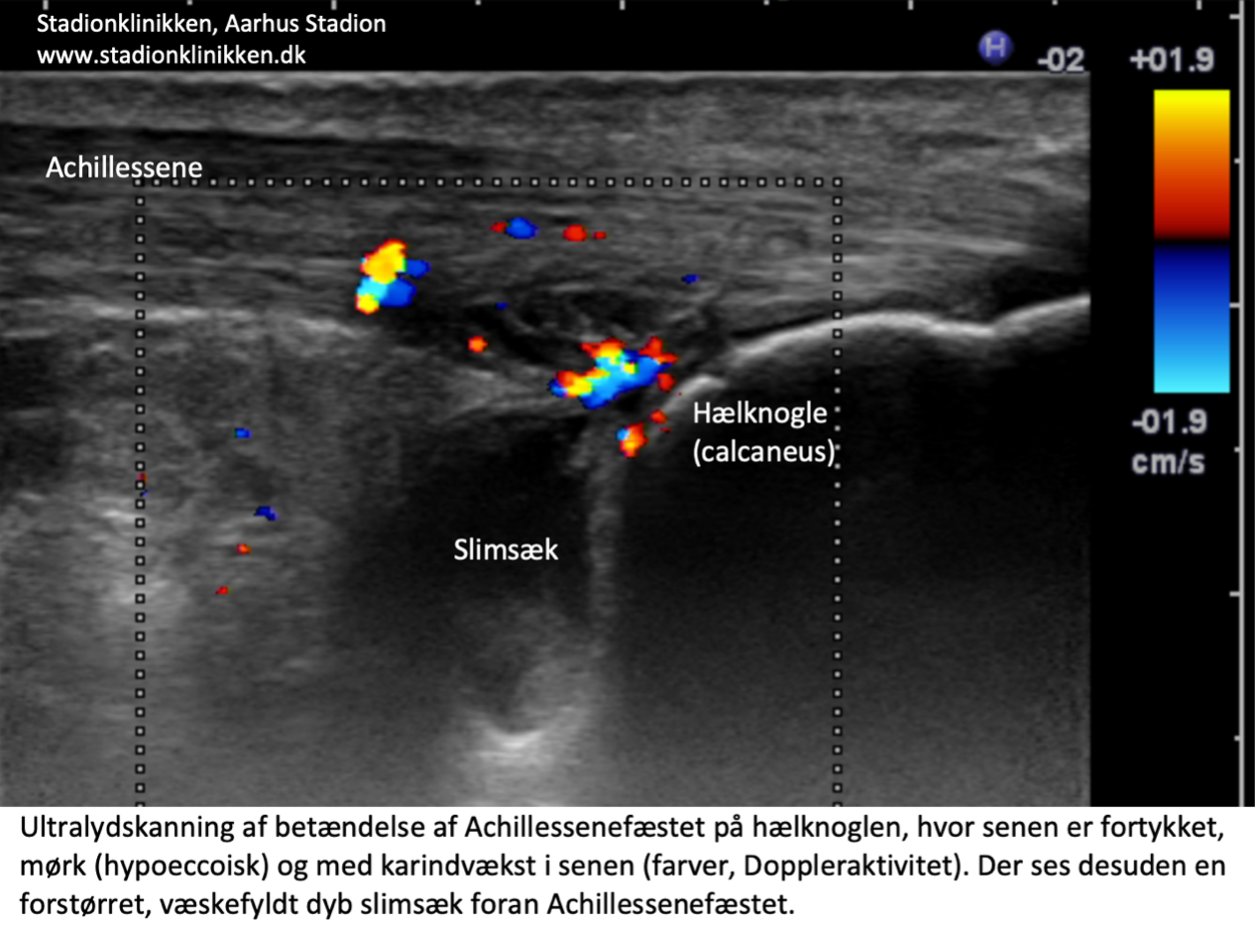
See image of Entesopatia Achilles and Bursitis Achilles
{kind=link}
{kind=link}
{kind=link}