Anatomy
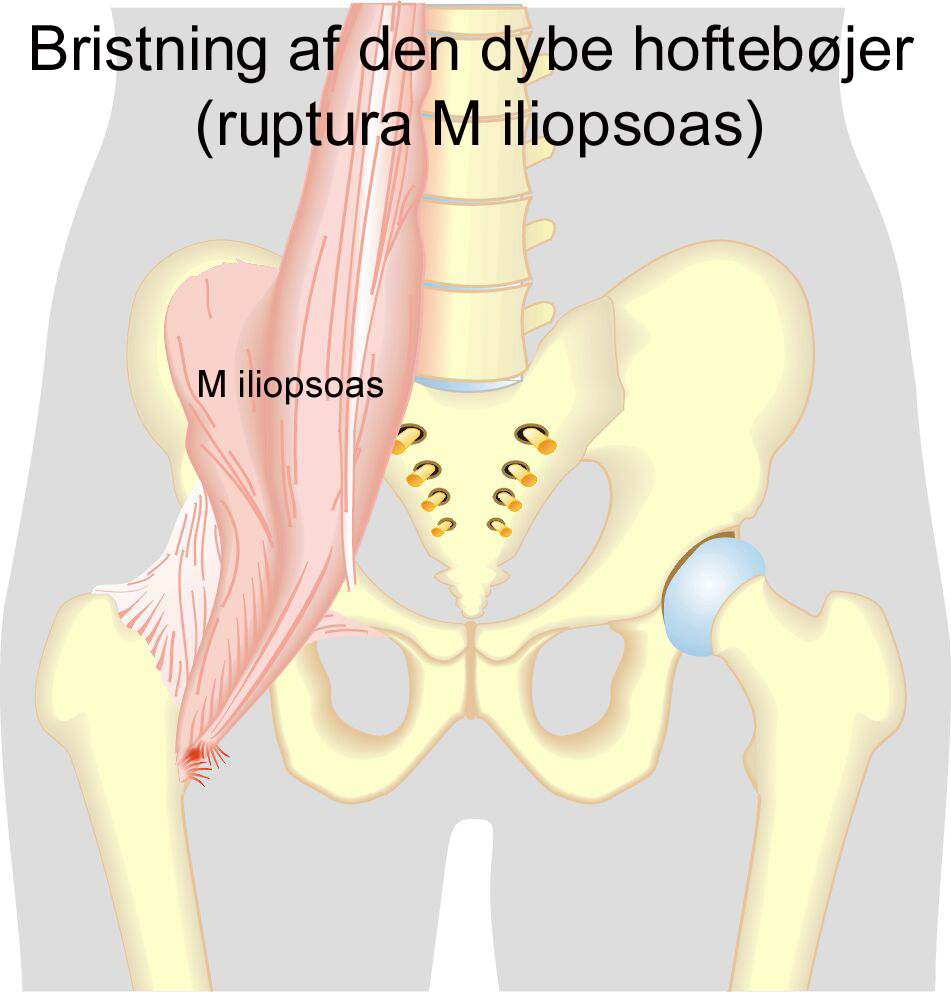
The deep hip flexor (M iliopsoas) consists of two muscles. The psoas muscle originates from the lumbar vertebrae and the iliacus muscle originates from the inside of the hip bone. The two muscles fuse together and both attach to the inside of the femur (trochanter minor). The iliopsoas is the strongest flexor muscle of the hip joint.
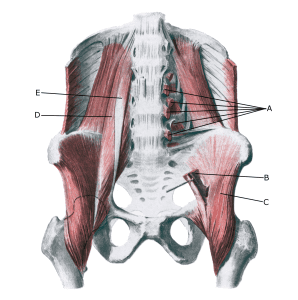
Pelvis from the front:
A. Origines m. psoatis
B. M. psoas major
C. M. iliacus
D. M. psoas major
E. M. psoas minor
See image of a deep hip flexor rupture
{kind=link}
{kind=link}