Anatomy
 Numerous nerves break through the abdominal wall and send nerve branches to the abdomen, groin and thigh area. The nerves can be pinched where they break through the abdominal wall. The sciatic nerve in the buttock can become pinched between the ischial tuberosity and the lesser trochanter
Numerous nerves break through the abdominal wall and send nerve branches to the abdomen, groin and thigh area. The nerves can be pinched where they break through the abdominal wall. The sciatic nerve in the buttock can become pinched between the ischial tuberosity and the lesser trochanter
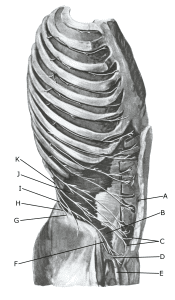
Nerves around the groin:
A. Umbilicus (navel)
B. M. obliquus internus abdominis
C. Rami cutanei anteriores n. intercostalis XII
D. Anulus inguinalis superficialis
E. Funiculus spermaticus
F. N. ilioinguinalis
G. N. iliohypogastricus (ramus cutaneus lateralis)
H. Ramus muscularis
I. N. iliohypogastricus
J. M. transversus abdominis
K. N. intercostalis XII