Anatomy
The pelvis consists of 2 halves, joined at the back by the sacrum and at the front by the pubic symphysis. The symphysis is not a true joint but consists of fibrous cartilage (fibrocartilago) that connects the two pubic bones. Only small rocking movements are possible. The abdominal muscle (M rectus abdominis) attaches to the pubic bone. The inner thigh muscles (e.g. M adductor longus) attach to the groin just below the pubic bone.
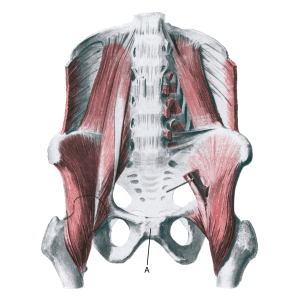
The pubic joint:
A. Symphysis pubica