Anatomy
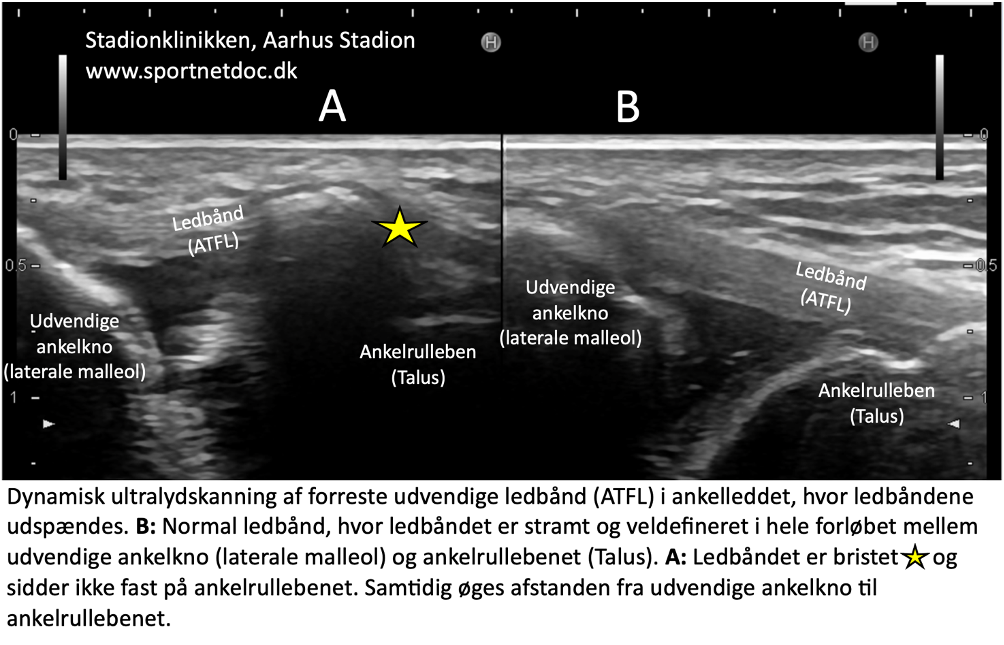
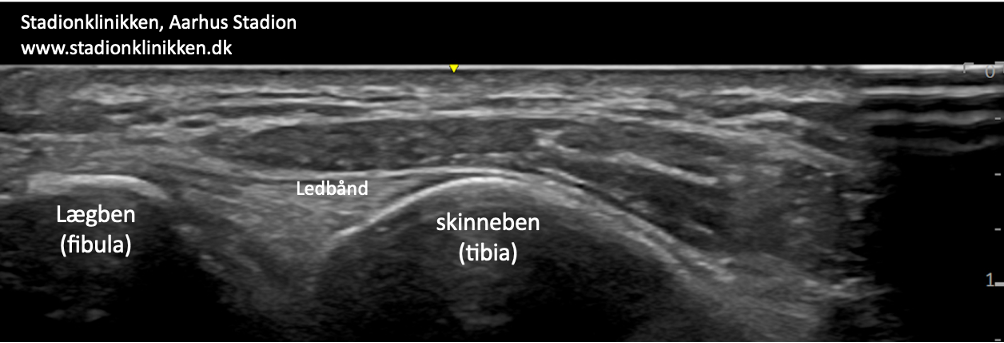
The ankle joint is stabilised by a joint capsule that is reinforced internally (medially) by a wide, fan-shaped ligament (ligamentum deltoideum) and externally (laterally) by 3 ligaments: an anterior (ligamentum talofibulare anterius), a middle (ligamentum calcaneofibulare) and a posterior (ligamentum talofibulare posterius). The ligaments stabilise the ankle joint, especially when twisting, running with changes in direction, etc. The tibia and fibula are held together in the ankle joint by 2 ligaments (ligamentum tibiofibulare anterius and posterius).
 Ankle joint, External
Ankle joint, External
A. Ligamentum mediale/deltoideum
B. Calcaneus
C. Talus
D. Tibia (Shin bone)
{kind=link}
{kind=link}
In particular
Rocking board exercises are important in both rehabilitation and prevention (Al Attar WSA, et al. 2023). Rocking board exercises should be performed regularly for the rest of the active sports career as a preventive measure if there is a history of ankle ligament injuries.
Start by standing with both feet on the balance board and supporting yourself with your hands against the wall. Gradually let go of the wall, and eventually practise balancing on just one leg.
You may wish to brush your teeth in the morning and evening whilst standing on the balance board (Wang F, et al. 2023).

